Download
1 / 1
10 likes | 162 Views
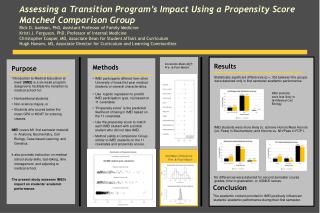
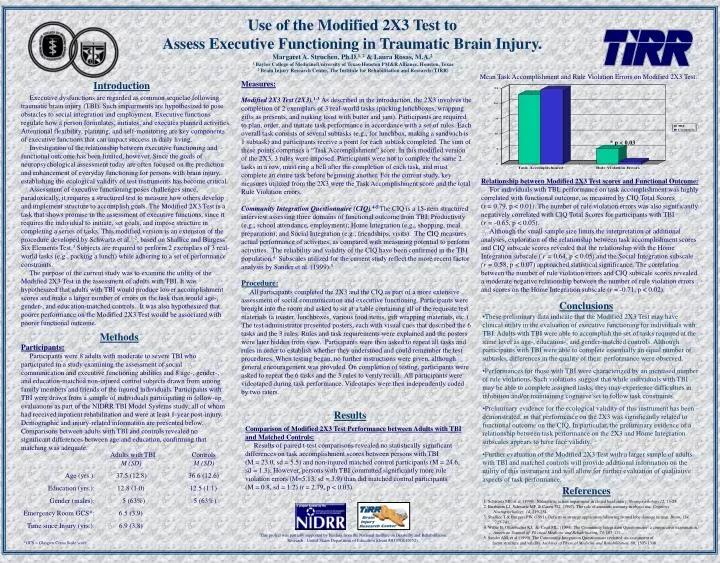
Mean Task Accomplishment and Rule Violation Errors on Modified 2X3 Test. Introduction. Measures:

E N D
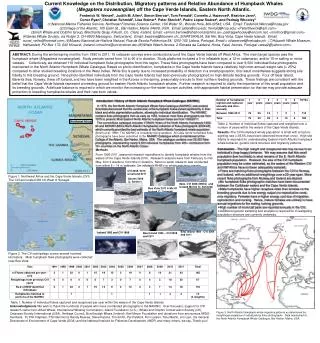
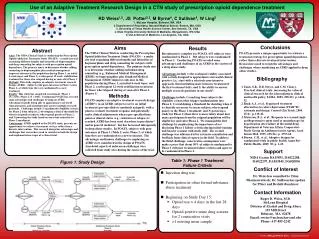
Mean Task Accomplishment and Rule Violation Errors on Modified 2X3 Test. Introduction Measures: Modified 2X3 Test (2X3).1-3As described in the introduction, the 2X3 involves the completion of 2 exemplars of 3 real-world tasks (packing lunchboxes, wrapping gifts as presents, and making toast with butter and jam). Participants are required to plan, order, and initiate task performance in accordance with a set of rules. Each overall task consists of several subtasks (e.g., for lunchbox, making a sandwich is 1 subtask) and participants receive a point for each subtask completed. The sum of these points comprises a “Task Accomplishment” score. In this modified version of the 2X3, 3 rules were imposed. Participants were not to complete the same 2 tasks in a row, must ring a bell after the completion of each task, and must complete an entire task before beginning another. For the current study, key measures utilized from the 2X3 were the Task Accomplishment score and the total Rule Violation errors. Community Integration Questionnaire (CIQ).4-5 The CIQ is a 15-item structured interview assessing three domains of functional outcome from TBI: Productivity (e.g., school attendance, employment); Home Integration (e.g., shopping, meal preparation); and Social Integration (e.g., friendships, visits). The CIQ measures actual performance of activities, as compared with measuring potential to perform activities. The reliability and validity of the CIQ have been confirmed in the TBI population.4 Subscales utilized for the current study reflect the more recent factor analysis by Sander et al. (1999).5 Procedure: All participants completed the 2X3 and the CIQ as part of a more extensive assessment of social communication and executive functioning. Participants were brought into the room and asked to sit at a table containing all of the requisite test materials (a toaster, lunchboxes, various food items, gift wrapping materials, etc.) The test administrator presented posters, each with visual cues that described the 6 tasks and the 3 rules. Rules and task requirements were explained and the posters were later hidden from view. Participants were then asked to repeat all tasks and rules in order to establish whether they understood and could remember the test procedures. When testing began, no further instructions were given, although general encouragement was provided. On completion of testing, participants were asked to repeat the 6 tasks and the 3 rules to verify recall. All participants were videotaped during task performance. Videotapes were then independently coded by two raters. Use of the Modified 2X3 Test to Assess Executive Functioning in Traumatic Brain Injury.Margaret A. Struchen, Ph.D.1, 2 & Laura Rosas, M.A.21 Baylor College of Medicine/University of Texas-Houston PM&R Alliance, Houston, Texas2 Brain Injury Research Center, The Institute for Rehabilitation and Research (TIRR) Executive dysfunctions are regarded as common sequelae following traumatic brain injury (TBI). Such impairments are hypothesized to pose obstacles to social integration and employment. Executive functions regulate how a person formulates, initiates, and executes planned activities. Attentional flexibility, planning, and self-monitoring are key components of executive functions that can impact success in daily living. Investigation of the relationship between executive functioning and functional outcome has been limited, however. Since the goals of neuropsychological assessment today are often focused on the prediction and enhancement of everyday functioning for persons with brain injury, establishing the ecological validity of test instruments has become critical. Assessment of executive functioning poses challenges since, paradoxically, it requires a structured test to measure how others develop and implement structure to accomplish goals. The Modified 2X3 Test is a task that shows promise in the assessment of executive functions, since it requires the individual to initiate, set goals, and impose structure in completing a series of tasks. This modified version is an extension of the procedure developed by Schwartz et al.1-2, based on Shallice and Burgess’ Six Elements Test.3 Subjects are required to perform 2 exemplars of 3 real-world tasks (e.g., packing a lunch) while adhering to a set of performance constraints. The purpose of the current study was to examine the utility of the Modified 2X3 Test in the assessment of adults with TBI. It was hypothesized that adults with TBI would produce lower accomplishment scores and make a larger number of errors on the task than would age-, gender-, and education-matched controls. It was also hypothesized that poorer performance on the Modified 2X3 Test would be associated with poorer functional outcome. * p < 0.03 Relationship between Modified 2X3 Test scores and Functional Outcome: For individuals with TBI, performance on task accomplishment was highly correlated with functional outcome, as measured by CIQ Total Scores (r = 0.79, p < 0.01). The number of rule violation errors was also significantly negatively correlated with CIQ Total Scores for participants with TBI (r = -0.65, p < 0.05). Although the small sample size limits the interpretation of additional analyses, exploration of the relationship between task accomplishment scores and CIQ subscale scores revealed that the relationship with the Home Integration subscale ( r = 0.64, p < 0.05) and the Social Integration subscale (r = 0.58, p < 0.07) approached statistical significance. The correlation between the number of rule violation errors and CIQ subscale scores revealed a moderate negative relationship between the number of rule violation errors and scores on the Home Integration subscale (r = -0.71, p < 0.02). Conclusions • These preliminary data indicate that the Modified 2X3 Test may have clinical utility in the evaluation of executive functioning for individuals with TBI. Adults with TBI were able to accomplish the set of tasks required at the same level as age-, education-, and gender-matched controls. Although participants with TBI were able to complete essentially an equal number of subtasks, differences in the quality of their performance were observed. • Performances for those with TBI were characterized by an increased number of rule violations. Such violations suggest that while individuals with TBI may be able to complete assigned tasks, they may experience difficulties in inhibition and/or maintaining cognitive set to follow task constraints. • Preliminary evidence for the ecological validity of this instrument has been demonstrated, in that performance on the 2X3 was significantly related to functional outcome on the CIQ. In particular, the preliminary evidence of a relationship between task performance on the 2X3 and Home Integration subscales appears to have face validity. • Further evaluation of the Modified 2X3 Test with a larger sample of adults with TBI and matched controls will provide additional information on the utility of this instrument and will allow for further evaluation of qualitative aspects of task performance. Methods Participants: Participants were 8 adults with moderate to severe TBI who participated in a study examining the assessment of social communication and executive functioning abilities and 8 age-, gender-, and education-matched non-injured control subjects drawn from among family members and friends of the injured individuals. Participants with TBI were drawn from a sample of individuals participating in follow-up evaluations as part of the NIDRR TBI Model Systems study, all of whom had received inpatient rehabilitation and were at least 1-year post-injury. Demographic and injury-related information are presented below. Comparisons between adults with TBI and controls revealed no significant differences between age and education, confirming that matching was adequate. Results Comparison of Modified 2X3 Test Performance between Adults with TBI and Matched Controls: Results of paired t-test comparisons revealed no statistically significant differences on task accomplishment scores between persons with TBI (M = 23.0, sd = 5.5) and non-injured matched control participants (M = 24.6, sd = 1.3). However, persons with TBI committed significantly more rule violation errors (M=5.13, sd = 3.9) than did matched control participants (M = 0.8, sd = 1.2) (t = 2.79, p < 0.03). Adults withTBIControls M (SD) M (SD) Age (yrs.): 37.5 (12.8) 36.6 (12.6) Education (yrs.): 12.8 (1.0) 12.5 (1.1) Gender (males): 5 (63%) 5 (63%) Emergency Room GCS*: 6.5 (3.9) Time since Injury (yrs.): 6.9 (3.8) *GCS = Glasgow Coma Scale score References 1. Schwartz MF, et al. (1998). Naturalistic action impairment in closed head injury. Neuropsychology,12, 13-28. 2. Buxbaum LJ, Schwartz MF, & Carew TG. (1997). The role of semantic memory in object use. Cognitive Neuropsychology, 14, 219-254. 3. Shallice T & Burgess PW. (1991). Deficits in strategy application following frontal lobe damage in man. Brain, 114, 727-741. 4. Willer B, Ottenbacher KJ, & Coad ML. (1994). The Community Integration Questionnaire: a comparative examination. American Journal of Physical Medicine and Rehabilitation, 73, 103-111. 5. Sander AM, et al.(1999). The Community Integration Questionnaire revisited: an assessment of factor structure and validity. Archives of Physical Medicine and Rehabilitation, 80, 1303-1308. This project was partially supported by funding from the National Institute on Disability and Rehabilitation Research , United States Department of Education (Grant #H133G010152).