Download
1 / 53
540 likes | 735 Views
LIPIDS. Study Guide Pg 171. Module Focus. Lipids are organic compounds that are insoluble in water They dissolve in organic solvents such as alcohol Hyperlipidemia is a biochemical state often associated with the development of atherosclerosis and coronary heart disease (CHD).

E N D
LIPIDS Study Guide Pg 171
Module Focus • Lipids are organic compounds that are insoluble in water • They dissolve in organic solvents such as alcohol • Hyperlipidemia is a biochemical state often associated with the development of atherosclerosis and coronary heart disease (CHD)
CLASSIFICATION OF LIPIDS • Fatty acids • Triglycerides • Cholesterol • Phospholipids • Lipoproteins
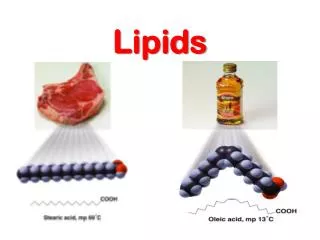
FATTY ACIDS Functions: • Metabolic energy • Building blocks for trigylerides & phospholipids • Not routinely measured
TRIGLYCERIDES Functions: • Main form of lipid storage • Provides energy for cell • Insulator of vital organs • Trigs are broken down by the enzyme lipase, epinephrine & cortisol • Trigs are transported in plasma as chylomicrons or VLDL
CHOLESTEROL • 75% Esterified form, 25% Free cholesterol Function: • Precursor of steroid hormones (estrogens, androgens) • Cell membrane structure • Formation of bile acids • Transported in plasma by LDL & HDL
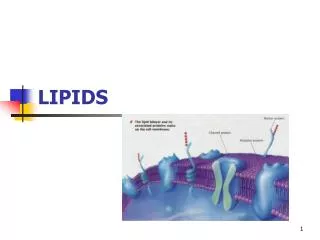
PHOSPHOLIPIDS Function: • Increases solubility of cholesterol • Forms a coating that surrounds cholesterol and triglycerides and glues the lipoprotein coreBilayer of cell membranes • Sphingolipids/sphingomyelin • Not measured routinely
LIPOPROTEINS • Lipid + Protein (apoprotein) • Protein provides an outer coating for the lipids making them soluble • Transports lipids in the plasma • Chylomicrons • Very low density lipoproteins (VLDL) • Low density lipoproteins (LDL) • High density lipoproteins (HDL)
LIPOPROTEIN METABOLISM • In the small intestine, food is digested by pancreatic enzymes and bile acids. • Fats (triglycerides) are hydrolyzed by lipase to fatty acids and glycerol. • They are absorbed & reassembled by the intestinal mucosa into new triglycerides, which are packaged into a structure called CHYLOMICRONS that provide a protein coating to make them soluble.
Chylomicrons enter the lymphatics and eventually reach the circulation. Peak triglyceride levels usually occur 30 – 90 minutes after a meal. • In the blood, chylomicrons are exposed to the enzyme lipoprotein lipase (LPL) on the surface of the endothelial cells. LPL hydrolyzes triglycerides into monoglycerides and fatty acids that can be absorbed by cells for energy and/or reassembled into trigs and stored in adipose tissue for future energy.
LPL leaves a chylomicron remnant that is taken up by the liver.
ENDOGENOUS PATHWAY • The liver is the principle site for endogenous lipid metabolism as well as apoprotein formation. • Triglycerides and cholesterol are packaged into triglyceride rich very low density lipoproteins (VLDL). • LPL hydrolyzes the VLDL trigs leaving an intermediate density lipoprotein (IDL
As triglyceride content decreases, cholesterol content increases, until the end product low density lipoprotein (LDL) is formed. • LDL is rich in cholesterol and transports cholesterol to tissues. • High Density Lipoprotein (HDL) is produced by the liver and intestine, it transports cholesterol from the cells back to the liver to be excreted.
LIPOPROTEINS • Chylomicrons • Very Low Density Lipoprotein (VLDL) • Low Density Lipoprotein (LDL) • High Density Lipoprotein (HDL)
FUNCTION • Essential for the transport of insoluble lipids in plasma • Provides cholesterol, phospholipids and triglycerides to tissues for: • Energy • Membrane synthesis • Hormone synthesis
LIPOPROTEIN STRUCTURE • Lipids + Protein • Inner core of lipids • Outer coating of protein to make them soluble in plasma PROTEIN COATING
CHYLOMICRONS • Not normally present in fasting specimens • Transport dietary lipids (exogenoustriglycerides) to body tissues • Responsible for most postprandial lipidemia • Major lipid = 95% trigs • Protein content = 1%
VERY LOW DENISTY LIPOPROTEIN “VLDL” • Transports body-made (endogenous) trigs to adipose tissue • 55% trigylcerides • 10% protein • Causes lipemia in serum specimens
LOW DENSITY LIPOPROTEINLDL • Major transporter of cholesterol • Transports cholesterol to tissues to be deposited • 45% cholesterol • 20% protein • levels associated with Coronary Heart Disease (CHD) Remember: Low density is “LETHAL”
HIGH DENSITY LIPOPROTEINHDL • Transports cholesterol from tissues to the liver to be excreted • Increased levels help prevent CHD • 50% protein • 20% cholesterol • 30% phospholipids
CLASSIFICATION LIPOPROTEINS
4 CLASSES BASED ON: • Electrophoretic mobility • Flotation characteristics: reference method • Chemical composition
ELECTROPHORETIC MOBILITY (+)Anode (-) Cathode CHYLOMICRONS ALPHA HDL BETA LDL PRE BETA VLDL
FLOTATION OR ULTRACENTRIFUGATION • The greater the protein content, the higher the density. • Current reference method chylomicrons VLDL LDL HDL
CHEMICAL COMPOSITION • Chylomicrons = dietary triglycerides • VLDL = body-made trigs • LDL = carries the “BAD” cholesterol • HDL = carries the “GOOD” cholesterol
CHOLESTEROL • Specimen requirements: • Fasting not required • No alcohol • No medications • No special diet for 2 weeks prior to analysis
METHODS OF MEASUREMENT • Abell-Kendall = current reference method • Utilizes Liebermann-Burchard reagent • Acetic anhydride & sulfuric acid • Not practical for routine use • Enzymatic is most commonly utilized
ENZYMATIC • Cholesterol esters are hydrolyzed to FREE cholesterol and fatty acids by the enzyme cholesterol esterase • FREE cholesterol is oxidized by the enzyme cholesterol oxidase to form hydrogen peroxide • The H2O2 reacts with a dye to form a colored compound.
REFERENCE RANGES • <200 MG/dl is desirable • 200 – 239 is borderline • > 240 is considered high risk
CLINICAL INTERPRETATIONIncreased Cholesterol • Coronary artery disease • Genetic defects in liver or lack of apoprotein B receptors on cell surface • Diabetes mellitus • Liver disease • Hypothyroidism • Nephrotic syndrome • Menopause due to estrogen • Increases in cholesterol levels do not change the appearance of plasma
TRIGLYCERIDES • Specimen requirements • 12 – 14 hr fast is mandatory • Nonfasting specimens = lipemic plasma due to the presence of chylomicrons which carry dietary trigs • Triglyceride levels peak 4 – 6 hrs after a meal
ENZYMATIC METHOD(detects glycerol) Lipase Trigs GLYCEROL + fatty acids • Trigs are hydrolyzed by lipase to form glycerol Glycerol dehydrogenase Glycerol + NAD NADH + dihydroxyacetone • Glycerol is quantitated by various methods
Reference Ranges • < 150- 200 mg/dl for a fasting specimen • 200 – 400 mg/dl = borderline high • >400 mg/dl = high
CLINICAL INTERPRETATION Increased Triglycerides • One of the most common causes is a nonfasting specimen • Oversynthesis • Diabetes mellitus, pancreatitis, alcoholism, obesity • Impaired catabolism – lack of lipoprotein lipase, present in capillary walls, it hydrolyzes trigs • Remember: increased trigs causes lipemia
HDL CHOLESTEROL The “GOOD” Cholesterol ? Remember:“H” is for healthy lower the risk of coronary artery disease • The higher the level of HDL, the lower the risk of coronary artery disease.
HDL METHODS • Precipitation of LDL, VLDL, and chylomicrons from serum specimen by the addition: • Phosphotungstate + MgCl2 or • Dextran sulfate + MgCl2
After centrifugation, HDL is the only lipoprotein remaining in the supernatant • A cholesterol method is then performed on the supernatant to determine the HDL HDL Cholesterol VLDL,LDL & Chylos
HDL Precipitation method is time consuming • Newer methods utilize immunoseparation techniques that do not require an extraction step.
CLINICAL INTERPRETATION • > 55 mg/dl = Low risk for CAD • < 40 mg/dl = High risk for CAD • HDL carries cholesterol from tissues to the liver for excretion
LDL CHOLESTEROL • The BAD cholesterol • Remember:“L” is for LETHAL • LDL carries cholesterol to tissues to be deposited • The higher the LDL, the greater the risk for CAD
LDL METHODS • LDL can be calculated: Total Cholesterol – (HDL chol + Trigs) 5 • Calculation is not very accurate if triglyceride measurement is nonfasting • Newer methods utilize immunoseparation and directly measure LDL
REFERENCE RANGE < 100 - 130 mg/dl
CLINICAL INTERPRETATION • < 100 -130 mg/dl = Low risk for CAD • 135 – 159 = Possible risk for CAD • > 160 = High Risk for CAD
VLDL CHOLESTEROL • Can be calculated by: TRIGYLERIDES 5 • Not very accurate
Total Cholesterol HDL Cholesterol RATIO • Divide the patient’s total cholesterol by their HDL cholesterol level Example: Cholesterol = 240 mg/dl HDL Cholesterol = 40 mg/dl • < 4 = Low risk for CAD • >5 = High risk for CAD 240 = 6 40
LIPOPROTEIN ELECTROPHORESIS Principle: Same as SPE. • Lipoproteins carry a net negative charge at a pH of 8.6 • Lipoproteins can be separated into 4 components CHYLOS PREBETA BETA Alpha - pole + pole
LPE Specimen: EDTA fasting plasma Support medium: agarose gel Lipid Stains: Oil Red O, Fat Red B, Sudan Black
CLINICAL INTERPRETATION • LPE is infrequently performed since total cholesterol, HDL, LDL & triglycerides provides sufficient information. • Normal SPE pattern: only alpha, beta & a small amount of prebeta will be visible • Chylomicrons should not be present in a normal fasting specimen