Download
1 / 32
460 likes | 1.36k Views
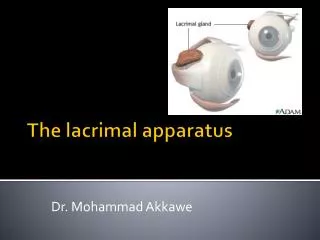
Anatomy and diseases of lacrimal apparatus. The lacrimal apparatus consists of -lacrimal gland -lacrimal passages Lacrimal gland –consists of 2 parts a)orbital lobe situated in a fossa in outer part of the orbital roof.

E N D
Anatomy and diseases of lacrimal apparatus The lacrimal apparatus consists of -lacrimal gland -lacrimal passages Lacrimal gland –consists of 2 parts a)orbital lobe situated in a fossa in outer part of the orbital roof. b)palpebral lobe situated in the outer part above the superior fornix. The ducts of the gland open in to the external part of the .superior fornix In structure the lacrimal gland resemble the salivary glands.
Lacrimal passages –consist of a) lacrimalpuncta: one in each lid and situated near the posterior border of the margin 6 mm from The medial canthus. b) Canaliculi : one in each eyelid-it commences at the punctum and carries tears to the lacrimal sac. c) Lacrimal sac : lies in the lacrimalfossa formed by the lacrimal bone and frontal process of maxilla.It is covered by lacrimalfoscia. Anterior to the lacrimalfoscia is the medial palpebralligament.The upper part of the sac is known as the fundus.The lower end narrows as it open into the nasolacrimal duct.
d)Nasolacrimal duct: It is 3-4 in length and opens into the inferior meatus of the nose. It is directed downwards,slightly outwards and backwards. The tears which are secreted by the lacrimal glands into the conjunctival sac are drained by the lacrimal passage into the nose.
Diseases of the lacrimal apparatus 1)Acute dacryoadenitis : occurs occasionally in general infection –mumps since the structure of the lacrimal gland is similar to the parotid and submandibular salivary glands. The gland becomes enlarged and tender. There is congestion and chemosis of the congunctiva. Treatment 1-Analgesic ,hot fomentation 2-Systemic antibiotics
2) Dacryops: It is a cystic swelling in the upper fornix due to retention of secretion owing to blockage of one of the lacrimal ducts. 3)Mikulicz's syndrome : is characterised by symmetrical enlargement of the lacrimal and salivary glands – parotid and submandibular . It is seen in cases of sarcoidosis , Hodgkins, disease, lymphoma, leukaemia, and tuberculosis . 4)Heerfordt's disease : In this disease uveitis is associated with enlarged parotid and lacrimal glands .
5)Tumoresof the lacrimalglands: owingto similarity of structure tumours of the lacrimal gland show a very marked resemblance to those of the partoid. The commonest one is pleomorphicadenocarcinoma or mixed tumour. It is seen in persons above the age of 40. There is proptosis and in addition the eyeball is pushed downwards and inwards.
Sjogren's syndrome or keratoconjunctivitissicca It is autoimmune disease seen in women after menopause and often associated with rheumatoid arthritis. Clinical features It is characterised by deficiency of the lacrimal secretion leading to dryness of the eye. There are chronic irritativesymptoms.The cornea shows superficial punctate or a filamentary keratitis. Damage to the epithelium of the conjunctiva and cornea may be demonstrated by staining pink with rose bengal.similar affection of the salivary glands may lead to dryness of mouth and the stomach .to achlorhydria
Sjogren's syndrome
:Treatment methyl cellulose drops or polyvinyl alcohol drops0.7% ( tear substitutes ) ; sealing of the lacrimalpuncta by secretion . diathermy in order to conserve
Watering of the eye 1)Epiphora : denotes watering due to obstruction .of outflow of tears a) Eversion of the lower punctum in ectropion of lower lid. b)Occlusion of the lower punctum -congenital -acquired cicatricial c) Occlusion of the lower canaliculus due to streptothrix, a scar, foreign body-eyelash,fungus, act inomyces , prolonged use of IDU . d)Chronic dacryocystitis
2-Lacrimation- reflex – causes due to sensory stimulation as in corneal ulcer ,exposure to smoke and irritant gases.
Chronic Dacryocystitis Etiology:It is usually due to an obstruction In the nasolacrimal duct, followed by infection of the lacrimal sac. 1) Obstruction of nasolacrimal duct a) Congenital impatency of the nasolacrimal duct due to imperfect canalisation of the epithelial cord particularly at the lower end. b) Tuberculosis, syphilis and leprosy - originating in surrounding bones or the nose. c) Structure of the duct due to chronic atrophic rhinitis. d) Obstruction of the lower end of the duct due to nasal polypi, hypertrophied inferior turbinate bone, extreme deviation of nasal septum. e) Maxilla - fracture, maxillary sinusitis, tumours of maxillary antrum. .f)Tumours of the lacrimal sac
2) Infection :stagnation of the content of lacrimal sac is quickly followed by Infection. As a result of contamination by micro - organisms from conjunctiva - staph, strept. and pneumococci a purulent inflammation of the lining of the sac is established. Symptoms: Epiphora increased by exposure to wind, cold, dust etc.
Signs: Sex incidence - it occurs more commonly in women. Age - most of the cases fall into the 40-60 years age group. In the female this coincides with the menopausal age and suggests a possible endocrine basis - hypertrophy of the mucous membrane which becomes more easily infected than usual leading to obstruction of the naso-lacrimal duct. 1) There may be pooling of tears near the medial canthus. 2) On pressure over the sac there may be a mucoid or mucopurulent regurgitation through the puncta or more rarely it passes down the nose. 3) There may be a non tender swelling at the site of the sac due to atony of its wall. This is called mucocoele. Sometime both the canaliculi may be blocked, when there is no regurgitation on pressure and the condition is known as encysted mucocoele.
Complications: 1) A form of chronic conjunct vitis affecting chiefly the caruncle and neighbouring parts of conjunctiva is frequent present-lacrimal conjunctivitis. Chronic dacryocystitis is an important cause of unilateral conjunctivitis. 2) Acute dacryocystitis may arise. 3) Lacrimal abscess. 4)Lacrimal fistula - when the lacrirnal abscess rupture or is drained.
5) The secretion from the sac Is most infectious and a constant source of danger to the eye with the risk of a hypopyon corneal ulcer should an abrasion of the cornea occur. 6) Orbital cellulitis, facial cellulitis and rarely cavernous sinus thrombosis. 7) Chronic dacryocystitis is an absolute contra indication to intraocular operatIon - such as cataract and glaucoma or account of the liability to infection (panophthaimitis). Therefore before undertaking any intraocular operation syringing of the lacrimal sac should be done.
Treatment: 1) In the new born a) Gentamycin drops b) Massage - The mother should be instructed to empty the sac by pressure several times a day. The little finger with the nail cut should be used. It should be done in such a with that the canaliculi are blocked by pressure of the finger again the orbital margin so that the fluid collected in the sac is forc down the nasolacrimal duct.
c) Probing of the naso lacrimal duct - to be done If marked improvement with the previous treatment. General anaesthesia is given. The punctum and canaliculi are dilat with a Nettleship’s dilator and a small probe is inserted vertical into the canaliculus. Great care is taken to avoid injuring the wall of the duct. The direction of the naso-lacrimal duct downwards, outwards and backwards. The passage of the probe once will cure most cases of congenital dacryocystitis.
2)In adults a) Cause of obstruction of the nasolacrimal duct should .be treated or removed if possible –nasalpoIyp b) Probing of the nasolacrimal duct is not indicated in :adults since it has a number of disadvantages 1)It is impossible to probe the swollen and inflammed.duct without injuring the wall .2)Such injury may lead to infection - acute cellulitis .3)Healing leads to fibrous stricture of the duct 4)Probing is painful .5)Most cases are benefited only temporarily
1)Dacryocystectomy (DCT) - As chronic dacryocystitis is a constant source of Infection, the lacrimal sac must be removed to prevent the development of hypopyon corneal ulcer. Epiphora usually persists for a time after excision of the sac but :gradually wears off since i) in normal condition the tears evaporate from the .surface of the globe ii) removal of the infected sac causes reflex inhibition .of tear secretion .Epiphora will still occur on exposure to wind
INDICATIONS FOR DCT 1)Chronic dacryocystitis in elderly person (above 60 years because : a) nasal mucosa is thin and atrophic ; it is difficult to .fashion flaps daring DCR . b) DCR is major operation - bleeding is more c) Lacrimal gland is atrophic - hence tear secretion is less. Therefore there are chances of dry eye developing if . DCR is done . 2)T.B. Syphilis or leprosy of the sac 3)Severe atrophic rhinitis (nasal muëosa is thin it is (difficult to fashion flaps during DCR .4)Tumour of lacrimal sac
Dacryocystectomy : . Is done under local anaesthesia . 1) 4 % xylocaine drops are instilled into conjunctival sac 2) 2% xylocaine with adrenaline is Injected over the area surrounding the sac .
Steps of operation : 1)A2 cm long curved incision is made with B.P. Knife (No.15) 3 mm medial to the inner canthus - care is taken not to injure the angular vein which lies 6-7 mm medial to the inner canthus . 2)The orbicularis muscle is split in the line of the incision and a lacrimal claw retractor inserted so as to retract it .with the skin 3)The medial palpebral ligament is cut at its attachment to . the anterior lacrimal crest
4)The lacrimal fascia is incised along the anterior lacrimal . crest, thus exposing the bluish sac 5) The sac is freed from the lacrimal fossa with the lacrimal dissector. The sac is twisted 2 or 3 times in artery forceps until it tears away from naso-lacrimal duct. The upper end of the naso-lacrimal duct is curetted with the .lacrimal curette
2)DCR-Dacryo-cysto-rhinostomy - In this operation the medial wall of the sac is anastamosed with the mucous membrane of the middle meatus of the nose, there by overcoming the obstruction at the junction of the lacrimal sac and nasolacrimal duct. The operation Is more physiological and there is no .resultant epiphora even on exposure to wind Indication : chronic dacryocystitis in young and middle aged person (below 60 years). Favourable cases are those with mucocoele
:Acute Dacryocystitis It occurs usually as an acute exacerbation of chronic dacryocystitis. Rarely it may start spontaneously. The same organisms like staph., pneumococci etc., which cause chronic dacryocystitis also give rise to acute .dacryocystitis : Symptoms 1)Fever 2)There is severe pain over the lacrimal sac .area radiating to the frontal region
:Signs 1)The skin over the sac becomes red, swollen, warm .an tender 2)The redness and swelling rapidly extend to the Iid and upper part of cheeks. 3)Congestion and chemosis of conjunctiva . 4)When lacrimal abscess is formed fluctuation can be elicited. The abscess usually points below owing to gravity and presence of medial palpebral ligament. When the abscess burst a lacrimal fistula is formed .
:Treatment 1)Analgesics/antipyretics such as paracetamol tablets. .2)Hot fomentation .3)Cap. amoxycillin 500 mg qid 4)If the lacrimnal abscess is pointing under the skin a small incision is made over the lower dependent part of the sac and the pus evacuated. After a few weeks a DCT or DCR may be done. NB: Syringing of lacrimal passages should not be done in acute dacryocystitis .
THANKS FOR YOUR ATTENTION Prepared by : Sami M. Shublaq