Download
1 / 57
570 likes | 832 Views
DEPRESSION. Peter M. Hartmann, M.D. Clinical Professor of Family and Community Medicine at Penn State College of Medicine June 23-25, 2011. Objectives. List criteria for major depressive disorder. Distinguish major depression from dysthymia and adjustment disorder.

E N D
DEPRESSION Peter M. Hartmann, M.D. Clinical Professor of Family and Community Medicine at Penn State College of Medicine June 23-25, 2011
Objectives • List criteria for major depressive disorder. • Distinguish major depression from dysthymia and adjustment disorder. • Provide optimal treatment for patients with depression.
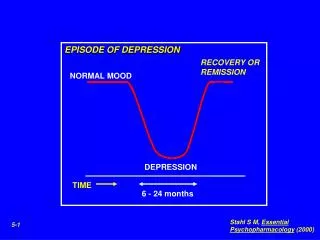
Essential Feature of MDD Patient must have either: Depressed mood (irritable in children) Or Loss of interest or pleasure For at least 2 weeks (Als0, must have at least 4 other symptoms.)
SIG E-CAPS • Sleep • Interest • Guilt (worthless) • Energy • Concentration • Appetite • Psychomotor agitation or retardation • Suicidal ideation
48 yo MWF high school teacher with MDD • Given paroxetine (Paxil) 20 mg X 6 weeks without benefit. • Changed to venlafaxine er (Effexor XR) 150 mg X 6 weeks also without benefit. What additional information do you want?
Has resistant depression. • Endorses the symptoms of MDD. • Was sexually abused as a child. • Is compliant with treatment. • TSH is normal. • Does not drink alcohol.
Causes of Resistant Depression • Wrong diagnosis (e.g., personality disorder) • Inadequate dose or length of treatment • Non-compliant • Substance abuse • Requires different treatment • Childhood abuse • Co-morbid dysthymia • Bipolar depression
Childhood Abuse • Rarely will antidepressants work alone. • Need to combine medication with therapy.
Bipolar Depression • History of mania or hypomania? • Family history of bipolar disorder, suicide, prolonged psychiatric hospitalization or non-schizophrenic psychosis.
Treatment of Bipolar Depression • Stop antidepressant if Bipolar I Disorder • Start mood stabilizer: • Lithium (level 0.6 to 1.2) • AED (lamotrigine good choice) • Atypical antipsychotic (quetiapine or aripiprazole)* • ECT * Only FDA approved are quetiapine XL and olanzapine/fluoxetine combined.
Major Depressive Disorder Resistant Depression
STAR*D Sequenced Treatment Alternatives to Relieve Depression (NIMH, 2876 patients, 6 years) • Majority fail to achieve & sustain remission (only 30%). • Cognitive behavioral therapy (CBT) = medication (CBT takes twice as long) • Start with citalopram; if no remission, proceed to sequenced treatments (Phase II – IV)
Phase I: Citalopram • Better response: Higher education Employed Married Caucasian Female Few complicating problems
Worse response: Co-occurring anxiety Substance abuse Physical illness Lower quality of life
Inadequate Response • Increase dose • Reinforce need to comply • Refer for therapy (cognitive behavioral or interpersonal) • Assess other factors such as diagnosis
Phase II • Three options if not in remission in 14 weeks: Option 1: Switch from citalopram to : • Sertraline • Bupropion SR • Venlafaxine XR • 25% remission • No difference among choices
Option 2: Augment • Bupropion SR • Buspirone • 33 1/3 % remission within 14 weeks • No difference in remission rate
Option 3: Cognitive therapy (CBT)* • Switch to CBT • Add on CBT • 23-25% remission • No difference between switch and add on • CBT = medication but takes twice as long *16 sessions over 12 weeks
Phase III • For the 50% not in remission after Phase II • Two options: Option 1: Switch up to 14 weeks • Mirtazapine • Nortriptyline • 10-20% remission • No advantage of one over the other
Option 2: Add different agent: • Lithium • T3 • 20% remission • Fewer SE with T3 (many dropouts with Lithium)
Phase IV • Take off all medications and change to one of 2 options: Option 1: Venlafaxine XR + Mirtazapine (10% remission) Option 2: Tranylcypromine (10% remission; more SE and harder to take)
Conclusions: • Switch from one SSRI to another. • Adding another agent helpful: Lithium Buspirone T3 Mirtazapine Bupropion Nortriptyline • Switch to Venlafaxine XR plus Mirtazapine • Switch to MAOi • Switch to or add CBT
Other Options from Different Studies: • Supplement with low dose atypical antipsychotic (e.g., aripiprizole 5 mg hs) • Methylphenidate or mixed amphetamine salt • Modafinil or Armodafinil • Folate may help depressed dementia patients • ECT, TMS, vagal nerve stimulation (Brain is electrochemical organ)
Bright Light • Dutch study of 89 outpatients, age 65 and older • 7500 lux of pale blue light for 1 hour in early AM vs. • 50 lux of dim red light for 1 hour in early AM (placebo) • Active > Placebo • Salivary cortisol down 34% with active vs. increase 7% with placebo.
SSRI PLUS ATOMOXATINEMichaelson et al J Clin Psych 2007; 68(4): 582
32 yo SWF secretary has been depressed “all my life;” low self-esteem; overeats and oversleeps; has therapist What additional information do you want?
More History • Sad mood most days for “my whole life” • Not anhedonic • Never had sex but libido seems normal to her • Never had suicidal thoughts • Mother and maternal aunt had major depression responsive to fluoxetine
Lab • TSH normal • Had polysomnography because of excessive sleeping. Results: • Decreased REM latency • Decreased slow wave sleep • Impaired sleep continuity • No PLMD or sleep apnea
Dysthymia • Chronically depressed mood most days for 2 years or more (one year in children) • At least two of the following: • Decreased appetite or overeating • Decreased sleep or oversleeping • Low energy • Poor concentration or trouble making decisions • Low self-esteem • Hopelessness
Considerations • Prevalence 6% (M:F is 2:1 in adults; kids 1:1) • Usually family Hx of MDD • Less vegetative symptoms than in MDD • “B,M,C” • “Double dippers” • 25-50% have same polysomnography as MDD • Cause of resistant depression
17 yo SF high school student broke up with boyfriend 2 weeks ago. • Cries “constantly” • Skipping classes • Won’t do her homework • Avoiding her friends • Mother reports she wishes she was dead What do you want to know?
More History • Does not meet criteria for MDD • Does not meet criteria for Acute Stress Disorder or PTSD • Has been a superior student who always did her homework and never missed class unless sick. • No substance abuse
Adjustment Disorder • Significant emotional or behavioral symptoms due to psychosocial stressor(s) within 3 months of onset of stressor(s) • Excessive distress or impaired social or occupational (school) functioning • Does not meet criteria for MDD • Does not apply if due to Bereavement • Symptoms last less than 6 months unless stressor(s) are continuing
Treatment • Therapy • Suicide is increased risk • Symptom relief based on clinical judgment (e.g., insomnia or anxiety) • No role for antidepressants unless also MDD
24 yo SBM with schizophrenia, bright, unemployed, c/o “depressed”
History • Distressed about cognitive difficulties and unemployment despite high IQ. • Lives with parents who are highly critical (negative expressed emotion). • Endorses sad mood, anhedonia, sleep and appetite decreased, never had much sex drive, poor concentration and self attitude, admits suicidal ideation.
Lab studies and Physical Exam • TSH normal • CBC, metabolic profile normal, elevated LDL • Urinalysis normal • Urine drug screen shows cannabis • Nicotine stains on fingers • Below ideal body weight
Treatment Considerations • Increased risk for relapse of schizophrenia due to parental negative expressed emotion. • High suicide risk (schizophrenia). • Pot smoking aggravating condition. • Cigarette abuse and limited self care. • Consider bupropion for depression and nicotine dependence. • Consider Omega 3 (4 capsules per day)
Stigma • Stress biological nature of MDD (just like diabetes) • Not your fault (allow yourself sick role) • Terry Bradshaw story
Bradshaw’s Story: • Born Sep 2, 1948 in Shreveport, Louisiana • Hyperactive and poor student as child • All American in college at Louisiana Tech • 6’3” 215 lb quarterback • Hall of Fame 1989 (broke all records) • Three time pro bowler with Steelers • 8 AFC Central Champs, 4 Super Bowl winners (MVP in 2)over 6 year timespan
Threw an 87 yard pass (AFC longest) • TV host, author, actor, singer, motivational speaker • Well known on “NFL Today” and “Fox NFL Sunday” • Married and divorced 3 times (2 kids to third wife) • “Bottomed out” at age 26 (marriage failed, shoulder injured, sullen and depressed)
Bradshaw and Depression • Frequent anxiety attacks after games • After 3rd divorce lost weight, crying spells, insomnia – diagnosed with depression and treated with Paxil • Is now a frequent speaker about men and depression. • Tries to destigmatize depression as an illness. • Is still in therapy and takes medication for ADHD.
25 yo MWF school teacher is 2 months pregnant. Presents with MDD. Prior Hx post partum depression.
More history • Meets criteria for MDD. • Not suicidal. • One male child age 6 with ADHD. • Supportive husband is worried about medications during pregnancy. • Had non-psychotic post partum depression successfully treated with sertraline.
Depression in Pregnancy • Depressive symptoms in 14-23 %. • Depression per se harms the fetus. • Depression assoc. with 2.5 fold increase in preeclampsia. • Goal is to optimize pregnancy outcome. • Encourage good health behaviors (prenatal vitamins, good eating habits, regular sleep, avoid alcohol and smoking).