Download
1 / 33
370 likes | 522 Views
Depression. Review of DSM-IV Criteria and Treatment Jamieson Bourque, MD, MHS Xavier Preud’homme, MD Editor: Amy Shaheen, MD, Assistant Professor of Clinical Medicine Duke University Medical Center. Epidemiology. Lifetime risk: Men: 7-12% Women 20-25%

E N D
Depression Review of DSM-IV Criteria and Treatment Jamieson Bourque, MD, MHS Xavier Preud’homme, MD Editor: Amy Shaheen, MD, Assistant Professor of Clinical Medicine Duke University Medical Center
Epidemiology • Lifetime risk: • Men: 7-12% • Women 20-25% • Increased prevalence in healthcare setting • 2-4% in general population, 5-10% in primary care office* • Lost productivity • estimated $31 billion/year cost in U.S. alone. • Risk of psychiatric co-morbidities • 61% have a co-occurring axis I condition • 30% have a comorbid axis II condition • 16-30% have a history of substance abuse *Katon, W, Schulberg, H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992; 14:237.
Epidemiology • Depression in the elderly associated with: • Significant healthcare costs • Functional decline • Effects on health outcomes: • Odds Ratio (O.R.) 3-4 for risk of one-year mortality in post-MI patients independent of other factors.* • O.R. 3.5 for 10-year mortality after CVA • Increased 1-year mortality on nursing home admission • Modified criteria for major depressive disorder found an O.R. of 7.8 for in-hospital mortality. *Frasure-Smith, N, Lesperance, F, Juneau, M, et al. Gender, depression, and one-year prognosis after myocardial infarction. Psychosom Med 1999; 61:26.
Risk Factors Major Risk Factors • Female gender • Prior history of depression • Family history of depression in 1st degree relative Associated Factors • Concurrent substance abuse • Childhood abuse • Stressful life event • Low self-esteem • Lack of social supports • Low-income • Middle-age
Etiology and Pathogenesis • Primary • Secondary • Neuropsychiatric: CVA, dementia • Endocrine: Hypothyroidism, diabetes mellitus • Medications: Corticosteroids, interferon • Rheumatologic: SLE, chronic fatigue syndrome, fibromyalgia • Other: • Cancer, especially pancreatic • Coronary artery disease • Hypercalcemia • Anxiety and panic disorders
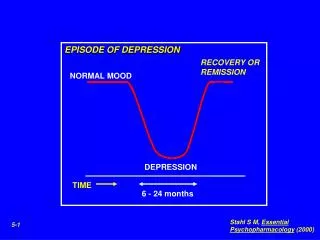
Definition and DSM-IV Criteria Major Depressive Disorder • 5 of the 9 criteria (next page) • At least one being depressed mood or anhedonia • Symptoms have been present for at least 2 weeks • Symptoms do not meet criteria for a mixed episode • Symptoms cause significant distress or impairment in social, occupational, or other areas of functioning • Symptoms are not due to a general medical condition or the direct psychological effects of a substance (drug/medication) • Although many of the same treatments apply even if the depression is secondary • Symptoms do not occur within 2 months of loss of a loved-one unless pathologic grief is present
Definition and DSM-IV Criteria 9 Major Criteria • Depressed mood (subjective or objective, such as tearful) • Anhedonia (markedly diminished interest or pleasure in almost all activities, reported or observed) • Significant weight or appetite loss or gain (weight >5% in one month) • Insomnia or hypersomnia • Psychomotor agitation or retardation (must be observed by others) • Fatigue or loss of energy • Feelings of worthlessness or guilt (may be delusional, not just self-reproach) • Impaired concentration, indecisiveness • Recurring thoughts of death or suicide
Definition and DSM-IV Criteria More Major Depressive Disorder Criteria • Must not be better characterized by a personality disorder • No history of mixed episode, manic or hypomanic episodes Recurrent Major Depressive Disorder • 2 single episodes with at least 2 months between where criteria were not met Mixed Depressive States • Depression with psychotic features • Depression with anxiety
Major Depressive Disorder Specifiers • Seasonal Affective Disorder • MDD episodes and full remissions occur regularly at a particular time of year • 2 MDD episodes related to season in the past 2 years with no episodes unrelated • Melancholia • Severe depression with somatic symptoms – particularly responsive to pharmacotherapy and ECT.
Associated Conditions • Grief/Bereavement • Response to loss of a loved-one. Typically resolves by 13 months. • Pathologic grief → MDD mixed with PTSD • Excessive worthlessness/guilt, symptom persistence, suicidality, intrusive images, avoidance behavior • Dysthymia • Chronic, low-intensity depression-like state with anhedonia, low self-esteem, and low energy • Symptoms must be present for at least 2 years • Bipolar Disorder • Diagnosed if the depressed patient has ever had a manic or hypomanic state • Different treatment is provided for depression in this state, especially to prevent rapid mood cycling • Atypical Depression (Depression NOS, “Mild depression”) • 2-4 MDD criteria for at least 2 weeks, often characterized by weight gain and hypersomnia. • 20% have significant social disability at 1 year
Depressed Mood or Anhedonia DSM-IV Criteria 5-9 2-4 Yes No <2 years ≥ 2 years Bipolar Disorder Major Depressive Disorder Depression NOS Dysthymic Disorder Classification Prior Manic Episode? Symptom Duration
Diagnostic Techniques • Screening – performed with 2 questions: • “Over the past 2 weeks, have you felt down, depressed, or hopeless?” • “Over the past 2 weeks, have you felt little interest/pleasure in doing things?” • Additional Workup (if either of the above are positive) • Ask specific/closed-end questions about the 9 diagnostic DSM-IV criteria • Ask about substance abuse and comorbid psychiatric conditions • Perform a medical ROS and medication history to rule-out secondary causes • Perform laboratory evaluation: • TSH, electrolytes, serum B12, folate, ECG • Assessment of suicide risk • Thoughts, intent, plan, means, prior attempts, family history
General Treatment Measures • Patient Education • Reassurance, associated physical symptoms, portrayal as a medical disease with a biochemical etiology. • Importance of medication compliance. • Exercise • May be effective in older adults • RCT of 156 pts ≥age 50 showed no difference over 16 weeks between 3x/week exercise, sertraline, or combination therapy. • ?Social interaction effect of exercise, highly motivated group • Phototherapy • May have an effect similar to pharmacotherapy in non-seasonal depression, but studies are limited and more research is needed. Blumenthal, JA, Babyak, MA, Moore, KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med 1999; 159:2349.
Psychotherapy • Multiple techniques: Cognitive behavioral, interpersonal, marital/family therapy, problem-solving treatment. • 12-20 weekly sessions • Efficacy in AHCPR 1993 Guidelines: • Cognitive, behavioral, interpersonal therapies: 46, 55, and 52 percent efficacy respectively.1 • Similar results in subsequent studies looking at these and problem-solving therapy. • Comparable efficacy to pharmacotherapy in RCT of 240 patients.2 • Sustained benefits – similar to that of patients maintained on pharmacotherapy. 1 Depression Guideline Panel. Depression in Primary Care: Treatment of Major Depression: Clinical Practice Guideline. US Dept of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR publication 93-0551, Rockville, MD 1993. 2DeRubeis, RJ, Hollon, SD, Amsterdam, JD, et al. Cognitive therapy vs medications in the treatment of moderate to severe depression. Arch Gen Psychiatry 2005; 62:409.
Medications Classes • TCAs • SSRIs • NDRI • SNRIs • NaSSA • SARI • MAO-Inhibitors • Herbal – St. John’s Wort
TCAs: Tricyclic Antidepressants • All tricyclics are negative allosteric modulators and therefore block both reuptake pumps for NE (norepinephrine) and 5-HT(serotonin) • The tertiary amines have more potency for inhibition of 5-HT than for NE (clonipramine, imipramine, amitriptyline) • The secondary amines have more potency for inhibition of NE than 5-HT (desipramine, nortriptyline) • Numerous side effects because all tricyclics block following receptors: - alpha1 adrenergic (dizziness, orthostatic hypotension & resulting falls) - H1 histaminergic (drowsiness & weight gain) - M1 muscarinic (constipation, worsening glaucoma, blurry vision, urinary retention, tachycardia) • All block Na channels and this has been the main reason for their cardiac toxicity such as QTc prolongation and risk for torsade de pointe (same as for class IA anti-arrhythmic)
SSRIs: Selective Serotonin Reuptake Inhibitors 1/3 • Selective and more potent inhibitors of serotonin reuptake than tricyclics • citalopram (Celexa), escitalopram (Lexapro), fluoxetine (Prozac) fluvoxamine (Luvox) paroxetine (Paxil) setraline (Zoloft) • No blockade of alpha1 adrenergic, histaminergic receptors nor Na channels • Slight antimuscarinic activity especially for paroxetine • There are numerous projections & types of serotoninergic postsynaptic receptors mediating as many functions as:- Mood (frontal cortex)- Akathisia/agitation, obsessions & compulsions (basal ganglia)- Anxiety & impulsivity (limbic structures)- Appetite, libido & temperature (hypothalamus)- Sleep (activating reticular formation)- Sexual dysfunction (spinal cord)- Nausea (brainstem and gut)
SSRIs: Selective Serotonin Reuptake Inhibitors 2/3 • Monoamine hypothesis stipulates that because of the deficiency in monoamine, some of these receptors are up-regulated in affective and anxiety disorders. Thus, once a SSRI is taken the increase in serotonin in the synaptic cleft is immediate and patient might experience side-effects before the benefits of the Rx kicks in, after the down-regulation of postsynaptic receptors occurs (which presumably takes about 2 weeks) • Side effects are: agitation & anxiety which may lead to impulsive suicide while mood remains hopeless, nausea, delayed orgasm • Too much serotonin leads to the serotonin syndrome with: myoclonus, diarrhea, confusion, hypomania, agitation, hyperreflexia, shivering, incoordination, fever and diaphoresis N Engl J Med 2005; 352:1112-1120, Mar 17, 2005
SSRIs: Selective Serotonin Reuptake Inhibitors 3/3 • In addition SSRIs are potent inhibitors of CYP 450 thus playing an important role in drug-drug interactions- CYP450 1A2: fluvoxamine (potent) - CYP450 2C9: fluvoxamine (potent), sertraline (weak)- CYP450 2C19: fluoxetine, fluvoxamine - CYP450 2D6: (es)citalopram (weak), fluoxetine (potent), fluvoxamine, paroxetine (potent), sertraline - CYP450 3A4: (nor)fluoxetine, fluvoxamine, sertraline (weak) • For the purpose of treating depression, all SSRIs offer comparable efficacy if prescribed for at least 4 weeks at their usual dose :- 10 mg for escitalopram- 20 mg for fluoxetine, paroxetine, citalopram- 50-100 mg sertraline- 100 mg fluvoxamine • However in anxiety disorders they are not all comparable (check FDA approval)
NDRI: Noradrenaline and Dopamine Reuptake Inhibitor • Bupropion is a weak dopamine and NE reuptake inhibitor (Wellbutrin) • Bupropion is metabolized into its hydroxylated active metabolite which is a potent NE reuptake blocker • Effective for patients who cannot tolerate side effects of SSRIs (or TCAs) such as sexual dysfunction or to nonresponders to SSRIs • May lower seizure threshold so contraindicated in patients with such known history as well as patients with eating disorders (probably because of the contribution of electrolytes imbalances to seizures) • Of course same molecule was also approved, though commercialized under a different name, for nicotine dependence (Zyban). For that matter consider starting the Rx 15 days prior to full cessation of smoking possibly in addition to the use of nicotine patch or other nicotine substitution
SNRIs: Serotonin and Noradrenaline Reuptake Inhibitors • Selective 5-HT and NE reuptake inhibitors • Prime examples are: venlafaxine (Effexor) and duloxetine (Cymbalta) • At usual therapeutic doses, little alpha1, muscarinic M1 or histaminergic H1 antagonisms. Yet because of their effect on the adrenergic system, the blood pressure is increased • SNRIs are like TCAs but without their usual side-effects. However at very high dose venlafaxine found to block the Na channel thus cardiotoxicity might still occur • Causes dual action on serotonin and adrenergic systems thus amplifying, in theory, theses two systems synergistically. Yet this has never been established by RTC trails • Thought to be good agents for SSRIs responders but not remitters • Venlafaxine antagonizes the NE reuptake above the dose of 150 mg daily, and therefore becomes a different antidepressant with an increase in its daily dose. In fact above 225 mg daily it becomes a weak inhibitor of the dopamine reuptake in addition to its effect on NE and 5-HT • Duloxetine seems to work on both 5-HT and NE at the same starting dose
NaSSA: Noradrenergic & Specific Serotoninergic ATD • Very different drugs devoid on any monoamine reuptake inhibition, yet increasing both NE and 5-HT • Prime examples are: mirtazapine (Remeron) and mianserin (Lerivon) though weaker • The mode of action is via a presynaptic alpha2 adrenergic antagonism that increases NE transmission on NE neurons but also 5-HT transmission on serotoninergic neurons • In addition, specifically block postsynaptically 5HT2A/C and 5-HT3 receptors thus reducing side effects such as anxiety, sexual dysfunction and nausea but also increases appetite (and often weight) and increases slow-wave sleep • Unfortunately also anti-histaminergic H1 and therefore induces drowsiness and also likely weight gain (and possibly metabolic syndrome) • Above a dose of 15 mg in hs, mirtazapine becomes a more activating medication via its increased adrenergic effect
SARI: Serotonin Antagonist/Serotonin Reuptake Inhibitor • Prime examples are trazodone (weak antidepressant) and nefazodone • Block selectively serotonin reuptake but in a less potent manner than tricyclics or even SSRIs • Also offer powerful post-synaptic 5HT2A/C antagonism which not only reduces the risks of classic SSRIs side-effects (anxiety, sexual side-effects) but also increases sedation and slow-wave sleep as well as as appetite (and thus weight) • In addition, blockade of 5HT2A/C receptors stimulate 5HT1A which may further help reduce depressive symptoms • Nefazodone though not a SSRI is a potent inhibitor of 3A4 (risk of rhabdomyolysis when combined with normal to high doses of statins, for example) • Some antimuscarinic side-effects and orthostatic hypotension with trazodone (be careful with elderly patients)
MAO-Inhibitors • Information given in case you manage a patient started on a MAOI by a specialist • MAO-A metabolizes 5-HT and NE selectively • MAO-B involved in metabolism of dopamine as well as amines acting as pro-toxins metabolized into toxins that may cause neuronal damages • Classic MAOIs are irreversible and non-selective meaning both the MAO-A and MAO-B enzyme activity cannot be restored unless new enzymes are synthesized: phenelzine, trancypromine, isocarboxazid • Such drugs are linked to blood pressure complications via the so-called “cheese effect” involving tyramine and leading to a surge in release of monoamines • RIMAs are antidepressant acting as reversible and selective inhibitors of MAO-A, such as moclobemide, presenting a safer profile in terms of paroxystic blood pressure elevation • Deprenyl is a selective MAO-B inhibitor
Herbal Remedies • The extracts from Hypericum perforatum L (St John's wort) have been shown to possess clinical efficacy in the therapy of mild to moderate depression although some negative reports exist as well (see Duke study by Davidson et al JAMA 2002; 287: 1807−1814) • Several in vitro studies have indicated that H. perforatum and its phloroglucinol constituent hyperforin act via a blockade of serotonin (5-HT), noradrenaline (NA) and possibly dopamine (DA) reuptake in a manner similar to most of the current antidepressant • Notably, St John’s wort is a potent inducer of the CYP450 1A2, 2D6 and 3A4 and this can lead to significant drug-drug interaction usually via loss of efficacy (i.e. OCPs and resulting pregnancies) • It can also be implicated in serotonin syndrome especially when combined with a SSRI
Medication Choice • Would start treatment with a SSRI or SNRI • NaSSA or NDRI would be reasonable alternatives for a moderate depression • For the treatment of depression, most ATDs are comparable • Yet, after more than 40 years of RTCs, amitriptyline remains slightly more efficacious with a NNT of 40 but a NNH of 8* • The choice of a medication should be based on your level of familiarity and also account for the anticipated side-effects profile and patient preferences • Given the availability of ATDs, would leave choice of a TCA or MAOI to a specialist and would not consider herbal treatment as first line agent * British Journal of Psychiatry 2001;178:129-44
Therapy Initiation and Monitoring • SSRI:-When initiating treatment with a SSRI, make sure the therapeutic dose is targeted (usually can be started directly at that dose, sometimes a quick 2-step titration may be preferred)- Close follow-up (weekly) is recommended at first especially if suicidal ideation is an issue (another reason to consider referral to a specialist)- Educating patient and family about time course of response is important as well as covering psychoeducation and information about side-effects • SNRI:- Remember they offer a different profile of side-effects (i.e. possible increase in blood pressure)- Venlafaxine works differently as dose is increased, at low dose though acts like a SSRI so same considerations for management of suicide risks apply
Treatment Duration • Critical because when sub-optimal treatment is provided or none, 50 to 85% of patients having a first episode will have at least one more subsequent one, with 10 to 20% developing a chronic course • The first episode should be treated for 6 months even when patient improves within the first weeks • Notably, the duration of treatment with an antidepressant for a depressive episode but in the setting of a a bipolar disorder is different and should also be referred to a specialist • When a patient has had at least 3 episodes of depression - unipolar, i.e. no (hypo)mania – long-term maintenance antidepressive therapy becomes the norm • Superior prophylaxis for patients who have suffered several recurrences is achieved with full-dose of active antidepressant medication compared to lesser doses
Refractory Depression • Really a matter for referral to a specialist:- Diagnosis might need to be reconsidered- Adjunct treatments may be needed- MAOIs and TCAs should be considered- Mood stabilizers might help- And of course, referral for ECT
Prognosis • Full remission in moderately depressed patients: • 46.4, 46.3 and 24.4% for pharmacotherapy, psychotherapy and placebo with 37.1, 22.2 and 54.4% of dropouts respectively* • Relapse/Recurrence: • 41% on placebo vs. only 18% on an active treatment** * American Journal of Psychiatry 2002;159(8):1354-60 ** Lancet 2003;361(9358:653-61
Conclusions • Efficacy between SSRIs and TCAs did not differ in a meta-analysis of trials restricted to primary care but significantly more patients on TCA withdrew specifically because of side-effects* • Choose an ATD based on your familiarity, side-effects profile, risks for adverse drug-drug interactions and patient’s preferences • SSRIs or SNRIs are probably best choices for non-psychiatrists • Support patient closely especially with initiation of treatment • Target the lowest therapeutic dose • Maintain treatment for at least 6 months if not longer in recurrent depression • Refer complicated, suicidal, refractory or bipolar cases to a specialist • British Medical Journal 2003;326(7397):1014
Please click here to complete the course evaluation References follow this slide