Download

1 / 21
210 likes | 391 Views
depression. in adolescence. Readings. Wenar, C. & Kerig, P. (2000)“ Disorders in the depressive spectrum and child and adolescent suicide in Developmental Psychopathology (pp. 143-159). Singapore: McGraw-Hill. Lecture Questions.

E N D
depression in adolescence
Readings • Wenar, C. & Kerig, P. (2000)“ Disorders in the depressive spectrum and child and adolescent suicide in Developmental Psychopathology (pp. 143-159). Singapore: McGraw-Hill
Lecture Questions • Where is the line between ‘normal’ adolescent depression and ‘abnormal’? • Why is adolescence a time of vulnerability to depression? • What does depression look like in adolescence? • What are the risk and protective factors for adolescent depression and youth suicide?
What’s ‘normal’? • Worrying • ‘Moodiness’ • ‘Puberty blues’ • Underdiagnosis related to ‘normal’ aspects of adolescence
Adolescent vulnerability Cognitive factors • Egocentricity • Black and white thinking • Emotional reasoning • Personal fable- uniqueness • Increased capacity for self awareness
Adolescent vulnerability • Adolescent ‘turmoil’ • Changing bodies, changing parental relationships • Sexual identities • Relationships • Academic pressures • Peer pressures • Balancing work and school
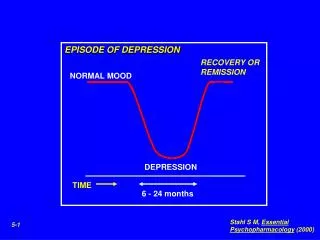
How common is it? • One of the three most common mental health problems in young people • First onset of a major depression often occurs in mid-late adolescence (15 mean age) • Rise in depression ages 13-15, peak ages 17-18, decline to adult levels • Depression is a significant problem for young people in custody or living on the streets • Episode in adolescence risk factor for episode in adulthood (Patton)
NZ prevalence • Fergusson & Horwood • 16-18 year old young women 30.2% rate • 18 plus 10.8% • 16-18 year old young men 13.7% • 18 plus 3.4%
Gender patterns • Onset of menarche significant for girls (around age 12) • Equal prevalence boys and girls til 15 then greater prevalence amongst girls (around twice as likely) • Girls’ depression predictor of subsequent episodes • Speculative differences in way depression differently expressed by girls and boys • Role of constructions of gender, pressures to conform with approach to adulthood
Adolescent presentation • Depressed mood Fatigue • Decreased concentration Insomnia • Social withdrawal Guilt • Negative self-image Anorexia • Anger/irritability Hopelessness • Suicidality Depression feels like falling out of a plane without a parachute I was often impatient with my friends. They didn’t want to be around me any more There aren’t any words to express the confusion of feelings
DSM Criteria • Persistent depressed mood • Loss of pleasure or interest in activities • Weight loss or gain • Insomnia • Restlessness • Fatigue • Feelings of worthlessness • Impairment in concentration, making decisions • Recurrent thoughts of death • 5 plus, two weeks at least 1 symptom (1) or (2)
Comorbidity • Substance abuse- Patton’s research on cannabis use • Anxiety disorders (60-70% in children) • Conduct disorder (boys) • Age patterns- preschoolers separation anxiety, school age children conduct disorder and adolescents eating disorders or substance abuse
Precipitating factors Relationship losses: • Girl/boyfriend • Family member • Close friend Failure to achieve a goal • Sports/leisure • Academic
Risk factors- young person • Biological changes • Physical illness • Poor nutrition • Alcohol or drug abuse • Negative self evaluation beliefs • External locus of control
Risk factors- family • Family history of depression • Early loss experiences • Exposure to non-optimal parenting experiences, especially focus on child’s failures or neglectful parenting • Lack of connectedness with family (Resnick et al.)
Risk factors-social • Stresses from e.g., sexuality issues, academic pressures, peer pressure, friendship/relationship problems, identitiy issues • Lack of connectedness with school (Resnick et al.)
Protective Factors • Resnick et al. “Protecting adolescents from harm” • Connectedness with family, other adults, or school • Religiosity • Feeling safe at school • Coping skills • Feelings of self-esteem and belonging • Secure cultural identity
Help-seeking Most young people don’t seek help: • Use informal versus formal help • Bullet proof-think they can handle it • Don’t know what’s available • Negative about what is available • Effects of depression itself • Psychosocial- levels of stress, confidence and social support
Youth Suicide • 1995 NZ worst rate of 13 OECD countries • 1998-140 deaths • 1999-120 deaths • 2000-96 deaths • Females attempt at twice the rate • Males higher ‘success’ • Maori males highest rate (numbers of suicides divided by population that age)
Key risk factors • High emotional distress • Previous attempts • Family/friend suicide attempt • Involvement in violence perpetration • Victim of violence • Substance abuse • Easy access to suicide ‘tools’
Protective factors • As for depression Resnick et al study: • No protective factors: 1 in 5 boys and 1 in 3 girls attempt • 3 protective and 3 risk factors: probability 4% boys, 8% girls • No risk factors, probability < 1% • Prevention + decrease risks and increae protective