Download
1 / 61
700 likes | 812 Views
Depression. DR.DUAA HIASAT. Objectives. Definition of depression . Signs & symptoms of depression according to DSM & ICD. Approach to depressed patient. Management. Assess suicidal risk in depressed patient. General principles. Mood: is a description of ones internal state of being.

E N D
Depression DR.DUAA HIASAT
Objectives • Definition of depression . • Signs & symptoms of depression according to DSM & ICD. • Approach to depressed patient. • Management. • Assess suicidal risk in depressed patient.
General principles • Mood: is a description of ones internal state of being. • Affect: the external display of ones mood. • Variation of mood is normal. • Mood disorders occurs when a patient's mood is not controllable and causes impairment in daily living activities.
Diagnostic & statistical manual of International classification Mental disorders of diseases & related health problem ( American psychiatric association) ( WHO )
Epidemiology of depression • Depression is highly prevalent among general population. • Mood disorders will be experienced by 9.5% of adults, MDD by 6.7% and BPD BY 2.6%. • Female more than males. • More if positive family history. • Mean age of onset Late 20s . • Depression is important in primary care. • Depression is usually under-recognised.
Etiologies & theories • GENETICS First degree relatives have three folds risk.
Etiologies & theories • PSYCHOSOCIAL FACTORS 1-recurrent stressful life events. 2-loss of parents before the age of 10. 3-living alone/lack of social support. 4-chronic pain. 5-alcohol & substance abuse. 6-medications. 7-vascular….post stroke, CAD.
Monoamine hypothesis • Most antidepressant medications increase the levels of one or more of the monoamines—the neurotransmitters serotonin, norepinephrine and dopamine—in the synaptic cleft between neurons in the brain. Some medications affect the monoamine receptors directly.
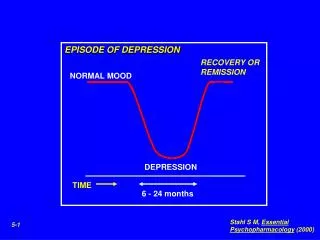
Depression- definition • Clinical syndrome of emotional, cognitive and physical symptoms associated with significant impacts on quality of life.
Common depressive disorders inprimary care • Major depression disorder ( MDD ). • Dysthymia. • Bipolar disorder. • Seasonal patterns. • Mood disorder secondary to a general medical condition.
Level of severity Sub-threshold depressive symptoms Fewer than 4 symptoms of depression Mild depression Few symptoms in excess of the 4,required to make diagnosis,& symptoms result in only minor functional impairment Moderate depression Symptoms & functional impairment s are BW mild & sever. Sever depression Most symptoms , & the symptoms markedly interferes with functioning. This can occurs with or without psychotic symptoms
Major depression disorder ( MDD ). • Chronic and relapsing, ccc by periods of exacerbation and remission. • Periods of remission can last years, but stressful events can bring out relapse. • Can cause significant impairment. • May occurein adolescents or latter in life.
Dysthymia • This is also known as chronic persistent depressive disorder. • More resistant to ttt . • Less likely to relieved by periods of remission or by antidepressant.
Seasonal pattern • Depression symptoms during winter months in regions that experience a marked decrease in ambient light during the winter. • Symptoms of hypersomnia, hyperphagia, & psychomotor slowing . • Hx of remission during summer months is helpful in the diagnosis. • Respond to high-intensity light therapy.
Screening • Because of high rates of unrecognized depression caseses. • USPSTF recommends screening adults for depression when staff-assissted depression care supports are available for accurate diagnosis, effective ttt, & follow-up. • USPSTF AGAINST screening…..
Screening • Conflicting recommendations, indicates the importance of proper monitoring & follow-up as mainstay of depression management.
Screening for… • People at risk of depression: • Hx of depression. • Significant physical illness causing disability. • Substance abuse. • Other mental health problems. • Complaintsthat involve multiple organ systems or are physiologically unrelated. • Sleep disturbance. • Frequent ER visits. • Patient who express thoughts or emotions that are inappropriate to the context.
Approach to depression • History taking. • Physical examination. • Lab investigation. • Differential Diagnosis. • Treatment.
History taking • Profile Age, gender, marital status. • Chief complaint • SIGECAPS. • Duration. S:sleep disturbance. I: decreased interest. G: guilt or worthlessness. E: decreased energy or fatigue. C: concentration poor. A: appetite or weight. P: psychomotor agitation. S: suicidal ideation. 2 weeks
History taking • Details about the symptom. • Other depression symptoms ( SIGECAP) 1:Mood----depressed 2:Sleep----increased or decreased 3:Interest----decreased 4:Guilt or worthlessness 5:Energy----decreased or fatigued 6:Concentration poor 7:Appetite or weight----increase or decrease 8:Psychomotor activity----increase or decrease 9:Suicidal ideation.
History taking • Diurnal variation. • Etiology of the problem ( emotional , financial, loss of job, home environment) • Post partum period. • First time or recurrent. • Seasonal pattern. • Other somatic symptoms( headache, back pain, SOB). • Other psychiatric illnesses.
History taking • Social history Loss of parents, living alone. • Medical history Chronic debilitating illnesses…. DM,HTN,Cancer,chronic pain. • Family history Three fold increase risk of depression.
Physical examination • General look General self neglection, no eye contact, self cutting marks…. • Mental status examination. • Vital signs. • Thyroid examination.
PSYCHIATRIC MANAGEMENT • Psychiatric management consists of interventions & activities that should be initiated & provided during all phases of treatment.
PSYCHIATRIC MANAGEMENT • Discussion & shared agreement. • Acute phase treatment ( psychotherapy, pharmacotherapy, ECT). • Evaluate response. • Continuation phase. • Maintenance phase. Monitoring to patient. • Discontinuation phase.
Cont….. • A strong trusting relation and therapeutic alliance btw ptn &dr, as this facilitates the stages of treatment. • Evaluate the safety of the patient by assessing the suicidal risk, if he demonstrates suicidal or homicidal ideation, close monitoring or hospitalization is needed.
Factors Increasing the Risk of Suicide in Depressed Patients 1. Increased age (70 years in men, 60 in women) 2. Gender (women make more attempts; men are more often successful) 3. Poor social support 4. Lack of marital support and absence of children 5. Chronic physical illness or chronic pain 6. Alcoholism or substance abuse 7. History of prior attempts 8. Specific plan or explicit communication about intent 9. Family history of successful suicide
Discussion & shared agreement • Consider the patient’s clinical condition including severity of symptoms or general medical conditions, level of functioning impairment. • Availability of supporting system. • Reliable feed-back process. • Enhance the treatment adherence by assessing the barrier to treatment, discuss concerns about tttor side effect. • Consider the patient’s preferences when modify or develop the treatment plane. • Encourage self-management activities. • Provide continuous education to the patient & family.
Acute phase treatment • Aim to induce remission of MDD & achieve a full return to patient baseline level of functioning. • Remission: at least 3weeks of absence of both depressed mood & inhedonia & no more than three remaining symptoms of MDD.
TREATMENT MODALITIES • Pharmacotherapy. • Psychotherapy. • Electroconvulsive therapy.
Contiu…. • Selection depends on : • Severity of the symptoms. • Co-occuring disorders or psychosocial stressors. • Biological , environmental factor at the current episode. • Patient preference. • Prior treatment experience.
Pharmacotherapy • Selective serotonin reuptake inhibitors(SSRI). • Tricyclic antidepressants(TCA). • Monoamine oxidase inhibitors(MAOI). • Reversible inhibition of MAO-A(RIMA). • Serotonin & norepinephrine reuptake inhibitors(SNRI). • Serotonin &dopamine reuptake inhibitors(SDRI). • Other cyclics (nefazodone).
Pharmacotherapy • Points to consider when selecting a medication include: • History of good response to previous use. • Successful use of an agent in a close relative (use by a parent or sibling may enhance compliance). • Presence of chronic pain or severe sleep disturbance (if so , consider using a TCA). • Coexisting medical conditions (e.g., avoid TCAs in patients with known cardiac conduction disturbances). • Hypersomnia (if so, consider an SSRI). • Cost. • Adverse effects and potential for drug interactions. • Patient preference.
Tricyclic antidepressants • Mode of Action : Block norepinephrine and serotonin Reuptake • Side Effects: Anticholinergic effects : dry mouth, blurry vision, acute glaucoma, constipation, urinary retention • Noradrenergic effects:tremors, tachycardia, sweating, insomnia, erectile and ejaculation problems • α-1 adrenergic effects: orthostatic hypotension • Antihistamine effects: sedation, weight gain • CNS: sedation, stimulation, decease seizure threshold • CVS: increased HR, conduction delay
SSRI • Block serotonin reuptake only • Side effects: Fewer than TCA, therefore increased compliance • CNS: restlessness, tremor, insomnia, headache, drowsiness • GI: N/V, diarrhea, abdominal cramps, weight loss • Sexual dysfunction: impotence, anorgasmia • CVS: increased HR, conduction delay, serotonin syndrome, EPS, • SIADH
SSRI • SSRIs inhibit P450 enzymes, therefore will affect levels of drugs metabolized by P450 system • Serotonin syndrome with MAOI: nausea, diarrhea, palpitations, hyperthermia, chills, neuromuscular irritability, altered consciousness