Download
1 / 24
300 likes | 1k Views
NEGATIVE SYMPTOMS IN SCHIZOPHRENIA. PRESENTER:- Dr. Bikramaditya Jaiswal. (INSTITUTE OF PSYCHIATRY- KOLKATA). Introduction. Definition. Evolution of the concept. Categories. Need for the division of symptoms. Types of negative symptoms. Deficit syndrome. Neuroimaging.

E N D
NEGATIVE SYMPTOMS IN SCHIZOPHRENIA. PRESENTER:- Dr. Bikramaditya Jaiswal. (INSTITUTE OF PSYCHIATRY- KOLKATA)
Introduction • Definition. • Evolution of the concept. • Categories. • Need for the division of symptoms. • Types of negative symptoms. • Deficit syndrome. • Neuroimaging. • Neurobiology of negative symptoms. • Neurobiological Correlates of specific Negative symptoms in Schizophrenia. • Scales. • Treatment • References.
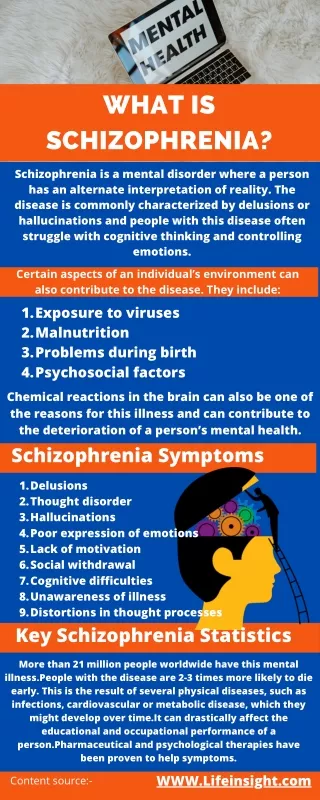
Definition • Represents a loss or diminution of normal functions [1]. • Behaviors which normals engage in but schizophrenics do not or only in diminished fashion[2].
Evolution of the concept • Kraeplin regarded what is today termed blunted affect and poverty of speech as permanent characteristics of Dementia praecox[4]. • Bleuler’s core or fundamental symptoms of schizophrenia included many negative symptoms[5].
Evolution of the concept • Strauss JS; Carpenter Jr., WT,Bartko JJ(1974) suggested that schizophrenic symptoms could be grouped in three relevant dimensions[6]. • Positive symptoms - disorders of content of thought and perception and certain behaviors. • Negative symptoms - blunting of affect, apathy, and certain kinds of formal thought disorder. • Disorders of relating - poor relationships and social avoidance.
Evolution of the concept • The positive/negative distinction was adopted by a number of investigators. • Three major models emerged: • Type I and Type II schizophrenia[7] (Crow, 1980) • Negative and Positive schizophrenia[8] (Andreasen and Olsen, 1982) • Deficit and Nondeficit forms of schizophrenia[9] (Carpenter Jr. et al., 1988). • Kirkpatrick et al.(1989) further specified deficit symptoms into deficit syndrome[10].
Categories • 5 general category :- • Avolition / Apathy. • Anhedonia. • Affective blunting / Flattening. • Passive or apathetic social withdrawal. • Alogia.
Need for the division of symptoms • Negative symptoms predict – • Worse quality of life • Worse social functioning • Worse interpersonal relationships • Worse work performance • Worse overall outcome
Negative symptoms Primary Secondary Secondary to drugs. Unrelieved positive sym. Depression Environmental hypo-stimulation Enduring (Deficit symptoms) Non – Enduring Deficit syndrome.
Primary negative symptoms comprise a core feature intrinsic to schizophrenia itself. • Least variable of the symptoms of schizophrenia. • Symptoms that do not diminish over the course of a year and do not remit with manipulation of the medication regimen should lead to consideration of primary negative symptoms.
Deficit syndrome –Presence of 2 or more (out of 6) negative symptoms -for a period of 12 months that are determined not to be secondary. • In comparison to Non –deficit group they have - • Poor prognosis • Lower quality of life, more time in hospital, increased frequency of symptomatic periods and more social and physical anhedonia. • Low IQ, less education, worse work history and poorer pre morbid social adjustment. • Respond poorly to medication or social skill training. • Less likely to have severe delusion, suspiciousness, suicidal ideation or attempts.
Neuroimaging • CT findings -Associations between negative symptoms and volume reductions in prefrontal cortical (PFC) including orbitofrontal (OFC), medial and lateral prefrontal cortices, temporal cortex, bilateral caudate, limbic and corpus callosum is found[11-16]. • Diffusion tensor imaging (DTI) studies - Association between negative symptom severity and abnormalities in orbitofrontal white matter tract integrity, internal capsule, corpus callosum, fronto-occipital fasciculus, left temporal lobe white matter tracts[17-18] • Functional neuroimaging findings - Relationship exists between negative symptom severity and reduced frontal metabolism[19-22].
Neurobiology of negative symptoms. • Winberger (1987) proposed dysregulation of dopamine system. • Putative hypofunction of prefrontal dopamine system could provide a possible neurobiological mechanism for negative symptoms • The combination of positive and negative symptoms common in schizophrenia could result from reduced prefrontal dopamine function, leading to relative hyperactivity of subcortical dopamine which would normally be modulated by prefrontal system.
Neurobiological Correlates of Specific Negative Symptoms in Schizophrenia • Role for the anterior cingulate volume in poverty of speech[23]. • Putamen and hippocampal involvement in affective flattening[24-25]. • Reductions in the activation of several prefrontal cortical regions and the ventral striatum in anhedonia[26]. • Reduced frontal lobe volumes and deficient activation of the ventral striatum in the context of amotivation[27].
Ant. cingulate Pre Frontal cortex Striatum Hippocampus
Scales for rating negative symptoms • Brief psychiatric rating scale (BPRS, Overall and graham 1962). • Scale for assessment of negative symptom (SANS, Andreasen 1989). • Positive and negative syndrome scale (PANSS, Kay 1987). • Schedule for deficit syndrome (Kirkpatrick et al, 1993).
Treatment • Pharmacological management[28-29]. • Assess factors that cause secondary negative symptoms. • Treatment of causes of secondary symptoms. • If don’t resolve by such treatments – consider primary negative symptoms. • Amisulpride, clozapine and olanzapine - tested for their efficacy against primary negative symptoms in selected cohorts. • Low dose Amisulpride – considered first line treatment for primary negative symptoms.
Treatment • Pharmacological management (contd.) • Aripiprazole and Olanzapine – 2nd line treatment. • Clozapine – not recommended for primary enduring negative symptoms. • Trials with NMDA agonists(Glycine, D-Cycloserine), Mirtazepine and SSRI – promising. • Mirtazepine, fluoxetine, fluvoxamine or paroxetine should be trialed as adjunctive medication in resistant patients. • One RCT showed reduction of negative symptoms with Mirtazepine augmentation of Risperidone.
Treatment • Psychosocial management[30]. • Activity-based therapy. • Cognitive-behavioural therapy (CBT). • Integrated therapy (IT).
References • Kaplan and saddock- comprehensive text book of psychiatry. • Joseph zubin – Negative symptoms : Are they indigenous to schizophrenia. • Berrios,G.E.. Positive and negative symptoms and Jackson- A conceptual history. Archives of gen. psychiatry. • Kraepelin E (1919) Dementia praecox and paraphrenia. Livingstone, Edinburgh • Bleuler E (1950) Dementia praecox or the group of schizophrenias. International Universities Press. • Strauss JS; Carpenter Jr., WT, Bartko JJ. An approach to the diagnosis and understanding of schizophrenia, part III. Speculations on the processes that underlie schizophrenic symptoms and signs. Schizophr Bull • Crow TJ. Molecular pathology of schizophrenia. More than one dimension of pathology? Br Med J 1980, • Andreasen NC, Olsen S. Negative versus positive schizophrenia: definition and validation. Arch Gen Psychiatry 1982; 39: 789-94. • Carpenter Jr. WT, Heinrichs DW, Wagman AMI. Deficit and nondeficit forms of schizophrenia: the concept. Am J Psychiatry 1988; 145: 578-83. • Kirkpatrick B, Buchanan RW, McKenny PD, Alphs LD, Carpenter Jr. WT. The Schedule for the Deficit Syndrome: an instrument for research in schizophrenia. Psychiatry Res 1989; 30: 119-24. • Baare WF, Hulshoff Pol HE, Hijman R, Mali WP, Viergever MA, Kahn RS (1999) Volumetric analysis of frontal lobe regions in schizophrenia: relation to cognitive function and symptomatology. Biol Psychiatry . • Hazlett EA, Buchsbaum MS, Haznedar MM et al (2008) Cortical gray and white matter volume in unmedicated schizotypal and schizophrenia patients. Schizophr Res 101 (1–3):111–123 • Koutsouleris N, Gaser C, Jager M et al (2008) Structural correlates of psychopathological symptom dimensions in schizophrenia: a voxel-based morphometric study. Neuroimage 39(4):1600–1612 • Sanfilipo M, Lafargue T, Rusinek H et al (2000) Volumetric measure of the frontal and temporal lobe regions in schizophrenia: relationship to negative symptoms. Arch Gen Psychiatry 57(5):471–480 • Wible CG, Anderson J, Shenton ME et al (2001) Prefrontal cortex, negative symptoms, and schizophrenia: an MRI study. Psychiatry Res 108(2):65–78
References 16. Young AH, Blackwood DH, Roxborough H, McQueen JK, Martin MJ, Kean D (1991) A magnetic resonance imaging study of schizophrenia: brain structure and clinical symptoms. Br J Psychiatry 158:158–164. • Wolkin A, Choi SJ, Szilagyi S, Sanfilipo M, Rotrosen JP, Lim KO (2003) Inferior frontal white matter anisotropy and negative symptoms of schizophrenia: a diffusion tensor imaging study. Am J Psychiatry 160(3):572–574 • Mitelman SA, Torosjan Y, Newmark RE et al (2007) Internal capsule, corpus callosum and long associative fibers in good and poor outcome schizophrenia: a diffusion tensor imaging survey. Schizophr Res 92(1–3):211–224. • Schroder J, Buchsbaum MS, Siegel BV, Geider FJ, Lohr J, Tang C, Wu J, Potkin SG (1996) Cerebral metabolic activity correlates of subsyndromes in chronic schizophrenia. Schizophr Res 19(1):41–53 • Volkow ND, Wolf AP, Van Gelder P, Brodie JD, Overall JE, Cancro R, Gomez-Mont F (1987) Phenomenological correlates of metabolic activity in 18 patients with chronic schizophrenia. Am J Psychiatry 144(2):151–158 • Wolkin A, Sanfilipo M, Wolf AP, Angrist B, Brodie JD, Rotrosen J (1992) Negative symptoms and hypofrontality in chronic schizophrenia. Arch Gen Psychiatry 49(12): 959–965 • Potkin SG, Alva G, Fleming K et al (2002) A PET study of the pathophysiology of negative symptoms in schizophrenia. Positron emission tomography. Am J Psychiatry 159(2): 227–237. • Makris N, Seidman LJ, Ahern T,Kennedy DN,Caviness VS, Tsuang MT, Goldstein JM (2010) White matter volume abnormalities &associations with symptomatology in schizophrenia. Psychiatry Res 183(1):21-29. • BallmaierM, Schlagenhauf F, Toga AWet al (2008) Regional patterns and clinical correlates of basal ganglia morphology in non-medicated schizophrenia. Schizophr Res 106(2-3):140– 147. • Szendi I, Kiss M, Racsmany M et al (2006) Correlations between clinical symptoms, working memory functions and structural brain abnormalities in men with schizophrenia. Psychiatry Res 147(1):47–55. • Harvey PO, Armony J, Malla A, Lepage M (2010) Functional neural substrates of self reported physical anhedonia in non-clinical individuals and in patients with schizophrenia. J Psychiatr Res 44(11):707–716.
References • Roth RM, Flashman LA, Saykin AJ, McAllister TW, Vidaver R (2004) Apathy in schizophrenia: reduced frontal lobe volume and neuropsychological deficits. Am J Psychiatry 161(1):157–159. • Drug treatment of the negative symptoms of schizophrenia : David .J. King; European neuropsychopharmacology 8 (1998) 33-42. • Pharmacological treatment of primary negative symptoms in schizophrenia. A systemic review; Schizophrenia research 88 (2006) 5-25. • Loving-Kindness Meditation to Enhance Recovery From Negative Symptoms of Schizophrenia David P. Johnson, David L. Penn, Barbara L. Fredrickson, and Piper S. Meyer University of North Carolina, Chapel Hill Ann M. Kring University of California, Berkeley Mary, Brantley Duke University.