Download
1 / 101
1.1k likes | 1.48k Views
OMM and the Athlete Upper Body Workshop. Jake Rowan DO Dept of OMM MSUCOM. Goals/Objectives. Review OPP and how they apply to sports medicine Discuss functional biomechanics Review palpatory dx Discuss OMM tx approach . An Osteopathic Approach to Treatment.

E N D
OMM and the AthleteUpper Body Workshop Jake Rowan DO Dept of OMM MSUCOM
Goals/Objectives • Review OPP and how they apply to sports medicine • Discuss functional biomechanics • Review palpatorydx • Discuss OMM tx approach
An Osteopathic Approach to Treatment • The role of the physician is to facilitate the healing process • The focus of treatment is the patient • The patient is treated in the context of the disease process they are experiencing. • The patient has the primary responsibility for his or her health. • There is a somatic component of disease and manipulative therapy can restore the body’s function, enhance wellness, and assist in recovery from disease and injury.
OPP - Manual Medicine Approach • Somatic Dysfunction • Impaired or altered function of related components of the somatic system (skeletal, arthrodial and myofascial structures) and the related vascular, lymphatic, and neural elements
Diagnostic Triad of Somatic Dysfunction • Asymmetry of position • Comparing left to right and superior to inferior • Range of motion restrictions • Standing Flexion Test • Stork Test • Seated Flexion Test • Tissue texture abnormalities • Change in soft tissue texture
MANUAL MEDICINE APPROACH • Physician needs to identify the problem, make the Dx, and Rx the appropriate TX • Tx – surgery, drugs, manipulation, therapeutic exercise • Goal for ManipulationTo improve mobility of tissues (bone, joint, muscle, ligament, fascia, fluid) and restore to normal physiological motion if possible. • Restore the maximal pain free movement of the musculoskeletal system in postural balance
MODELS OF MANUAL MEDICINE • Biomechanical model. • Neurologic model. • Respiratory-circulatory model. • Bioenergy model. • Organ system model.
Models, Mechanisms & Activating Forces • Model relates to the therapeutic objective of the intervention. • Method relates to the approach to the restrictive barrier. ( Direct, Indirect, Combined). • Depends on the clinician, patient and environment/setting • Activating Forces - intrinsic and extrinsic.
JOINT PLAY • Definition: Movement within a synovial joint that is independent of, and cannot be reproduced by, voluntary muscle contraction, but essential for maximal pain free movement of the joint. • Joint examination: Examination is made for the precise joint play movements of that joint. • Joint treatment/manipulation: Movements that restore joint play. • Occurs in all synovial joints.
John McM. Mennell, M.D. Physiatrist trained at Cambridge England. His father James also a manual medicine physician. They introduced Joint Play examination & treatment. One of founders of NAAMM.
JOINT DYSFUNCTION • A specific type of somatic dysfunction • The loss of joint play movement that cannot be recovered by voluntary muscle. • Normal voluntary movements are restricted and frequently painful.
JOINT PLAY EVALUATION & THERAPEUTIC MANIPULATION • Evaluate each play movement and compare with contralateral side. • Therapeutic manipulation is the use of a high velocity, low amplitude thrust to restore the play movement.
THE “NEVERS”IN JOINT PLAY EVALUATION • Normal ligaments are NEVER tender to palpation. • You can NEVER palpate a normal joint capsule. • You can NEVER palpate fluid in a normal joint. • NEVER manipulate a swollen, warm, or inflamed joint.
10 RULES OF JOINT PLAYEXAM & TREATMENT • Patient must be relaxed. • Therapist must be relaxed. Therapeutic grasp must be painless, firm, and protective. • One joint mobilized at a time. • One movement in a joint restored at a time. • One aspect of the joint is stabilized and the other aspect moved. • Extent of movement is same as assessed in the same joint on the opposite side. • No forceful or abnormal movement must ever be used. • The manipulative movement is a sharp thrust, with velocity, to result in a 1/8th“ gapping or sliding at the joint being treated. • Therapeutic movements occur when all of the “slack” has been taken up in the joint. • No therapeutic maneuver is done in the presence of joint or bone inflammation or disease (Heat, redness, swelling, etc.).
Tx Approach Principles • Treat the axial skeleton first • Extremities: start proximal work distal • LE – pelvis, hip, knee, ankle, foot, toes • UE – scapula, SC, AC, glenohumeral, elbow, wrist, hand, fingers
Tx Approach Principles • Motor Control • Balance • Core stability • Stretch before strengthening
Tx Approach Principles - Neck • Thoracic spine • Ribs • Structural & functional • Scapula • Cervical spine • Cranium • OA jt • Muscle imbalance
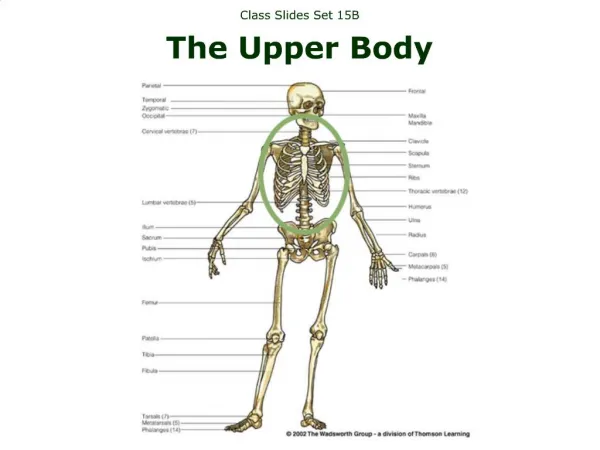
Tx Approach Principles - UE • Thoracic spine • Ribs • Scapula • Cervical spine • SC, AC, glenohumeral, elbow, wrist, hand
Anatomy of the Scapula and Posterior ShoulderThe Quadrangular Space
SCAPULAR ROTATION ON THE THORAX • Athlete’s arm on your shoulder • Fingers under medial edge of blade • Both hands move scapula medially, laterally, superiorly and inferiorly • Athlete breathes through maneuvers
STERNOCLAVICULAR JOINT • Articular capsule & disc. • Anterior sternoclavicular ligament. • Posterior sternoclavicular ligament. • Interclavicular ligament. • Costoclavicular ligament.
Sternoclavicular Joint Diagnosis Test for Restricted Abduction • Patient supine on table with arms resting easily at the side. • Operator stands at side or head of table with paired fingers over the superior aspect of the medial end of the clavicle. • The patient is asked to actively ‘shrug the shoulders’ by bringing the shoulder tip to the ear bilaterally. • The operators palpating fingers follow the movement at the medial end of the clavicle.
Sternoclavicular Joint Diagnosis Test for Restricted Abduction • The normal finding is equal movement of the medial end of both clavicles in a downward direction. • A positive finding is the failure of one clavicle to move downward when compared to the opposite. It appears to be held in the original starting position. • Note: This test can also be done with patient sitting.
Sternoclavicular Joint Muscle Energy Technique Supine • Operator internally rotates the dysfunctional upper extremity and carries it into extension off the edge of the table to the resistant barrier while monitoring with the opposite hand at the sternoclavicular region • Patient performs a 3-to 5-second muscle contraction to lift the arm toward the ceiling against operator resistance for 3 to 5 repetitions. • Following each relaxation, the operator increases the extension of the upper extremity to a new resistant barrier and patient again repeats the effort of lifting the arm toward the ceiling.
Sternoclavicular Joint Muscle Energy Technique Sitting • Patient sitting on table or stool. • Operator standing behind patient with the thenar eminence of one hand in contact with the superior aspect of the medial end of the dysfunctional clavicle and the other hand controlling the dysfunctional upper extremity at the elbow • With the elbow at 90 degrees, the upper extremity is externally rotated and abducted to approximately 90 degrees with additional abduction until the resistant barrier is engaged
Sternoclavicular Joint Muscle Energy Technique Sitting • Patient performs muscle contraction to adduct the upper extremity three to five times for 3 to 5 second against resistance offered at the elbow by the operator. • After relaxation, operator engages new barrier.
RESTRICTED ABDUCTION OF SC JOINT caudal pressure on clavicle sweep arm to opposite knee
Sternoclavicular Joint Diagnosis Test for Restricted Horizontal Flexion • Patient supine on table. • Operator stands at side or head of table with fingers symmetrically placed on the anterior aspect of the medial end of each clavicle • Patient extends the upper extremities in front of the body by reaching toward the ceiling • Operator evaluates movement of the medial end of each clavicle • The normal finding is for each clavicle to move symmetrically in a posterior direction as the lateral end of the clavicle moves anteriorly • A positive finding is for one clavicle not to move in a posterior direction during the reaching effort
Sternoclavicular Joint Muscle Energy Technique Supine • Patient supine on table. • Operator stands on side of table opposite the dysfunctional sternoclavicular joint. • Operator places one hand over the medial end of the dysfunctional clavicle and the caudad hand grasps the patient’s shoulder girdle over the posterior aspect of the scapula • Patient’s hand grasps back of operator’s neck with an extended arm
Sternoclavicular Joint Muscle Energy Technique Supine • Operator engages the horizontal flexion barrier by standing more erect and lifting the dysfunctional scapula • Patient pulls down upon the operator’s neck with 3 to 5 second muscle effort for 3 to 5 repetitions while operator maintains posterior compression on the anterior aspect of the medial end of the dysfunctional clavicle. • Operator engages new barrier after each of patient’s muscular contraction
RESTRICTED HORIZONTAL FLEXION OF SC JOINT posterior pressure on clavicle arm sweeps from horizontal extension to flexion
ACROMIOCLAVICULAR JOINT • Superior acromioclavicular ligament. • Inferior acromioclavicular ligament. • Coracoclavicular ligament.
Acromioclavicular Joint Test for Restricted Abduction and Adduction • Patient sitting with operator standing behind. • Operator’s medial hand palpates the superior aspect of the ac joint monitoring a gapping movement at the ac joint and the lateral hand controls the pt’s proximal forearm and takes pt’s upper extremity to horizontal flexion of 30 degrees then adds ADduction and ABduction. • Absence of the gapping movement is evidence of restriction of adduction or abduction movement. • Comparison is made with the opposite side.
Muscle Energy Technique Sitting Tx: Restricted Abduction • Patient sitting on table or stool with operator standing behind. • Operator maintains compressive force on lateral end of the clavicle, medial to the ac joint. • Operator’s lateral hand takes patient’s upper extremity to horizontal flexion of 30 degrees and abducts to the barrier • Patient pulls elbow to the side against resistance offered by the operator for 3 to 5 seconds and 3 - 5 repetitions. • Operator engages new abduction barrier after each muscle effort
Acromioclavicular Joint Diagnosis: Test for Restricted Internal and External Rotation • Patient sitting on table or stool with operator standing behind. • Operator’s medial hand palpates the superior aspect of the ac joint. • Operator’s lateral hand moves the upper extremity into horizontal flexion to 30 degrees and abduction to the first barrier
Acromioclavicular Joint Diagnosis: Test for Restricted Internal and External Rotation • Operator introduces internal rotation and external rotation while monitoring mobility of the ac joint. • Comparison is made with the opposite side
Muscle Energy Technique Tx: Restricted External Rotation • Operator’s medial hand stabilizes the lateral aspect of the clavicle and monitors the ac joint. • Operator takes upper extremity to 30 degrees of horizontal flexion and abduction to 90 degrees. • External rotational barrier is engaged with the operator’s lateral hand grasping the patient’s wrist and places forearm to patient’s forearm
Muscle Energy Technique Tx: Restricted External Rotation • Patient provides muscle contraction for 3 to 5 seconds and 3 - 5 repetitions against resistance of external rotation. • Operator engages new barrier after each muscle contraction.
Muscle Energy Technique Tx: Restricted Internal Rotation • Operator’s medial hand stabilizes the lateral aspect of the clavicle and monitors the ac joint. • Operator takes upper extremity to 30 degrees of horizontal flexion and abduction to 90 degrees. • Operator engages internal rotation barrier by threading lateral forearm under patient’s elbow and grasping distal forearm
Muscle Energy Technique Tx: Restricted Internal Rotation • Patient provides muscle contraction for 3 to 5 seconds and 3 - 5 repetitions against resistance of internal rotation. • Operator engages new barrier after each muscle contraction.
SHOULDER JOINT BURSAE • Subdeltoid bursa. • Subacromial bursa. • Deltoid. • Supraspinatus. • Acromion & coracoacromial ligament.