Measles
Measles. 30-40 million cases a year worldwide 750,000 deaths (WHO 2002) – half in Africa Accounts for about half of all vaccine preventable deaths. Measles. Morbillivirus of Paramyxovirus family Transmission through fine and large droplets Incubation 7-18 days

Measles
E N D
Presentation Transcript
Measles • 30-40 million cases a year worldwide • 750,000 deaths (WHO 2002) – half in Africa • Accounts for about half of all vaccine preventable deaths
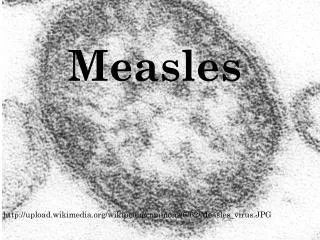
Measles • Morbillivirus of Paramyxovirus family • Transmission through fine and large droplets • Incubation 7-18 days • Early symptoms: fever,coryza, conjunctivitis, cough, malaise • Koplik’s spots
Measles • Rash – erythematous, maculopapular
Measles • Infectious from start of symptoms until 4 days after the rash appears, very highly infectious R = 17 • Common complications of Measles are otitis media, pneumonia, diarrhoea and convulsions • Rare complications are encephalitis and SSPE
2 dose MMR • About 90% children develop immunity to Measles after 1 vaccination • In order to maintain high enough levels of herd immunity to prevent transmission need 2 doses of MMR • Finland introduced a 2 dose strategy in 1982, the US introduced one in 1989
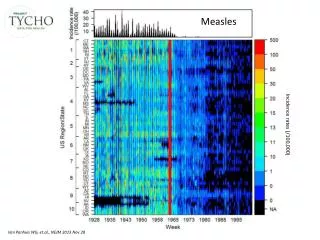
Measles British Isles • In UK, from 1940 to 1968, Measles in 2 yearly cycles with between 160,000 and 800,000 cases/yr • Single Measles introduced in 1968 • MMR introduced in 1988 • No deaths since 1992 • 1994 MR campaign, 8 million vaccinated aged 5 -16 • 1996 2nd dose MMR introduced
At risk groups • Immunocompromised individuals • Infants under 1 yr of age • Pregnant women at any stage of gestation
Interventions • Proactive immunisation, coverage needs to be 95% or more to prevent outbreaks as population immunity of 90% is required and vaccine is about 90% effective • Lower levels of population immunity will limit spread
Reactive interventions • Immunisation with MMR, if given within 72 hrs of first exposure, currently recommended in children over the age of 6 months • HNIG, for immunosuppressed, younger infants and pregnant women • School exclusion
Case definitions • Confirmed case, compatible rash illness with either serological evidence of recent Measles infection or PCR identification of Measles virus • Probable case, compatible illness and epidemiological link to confirmed case • Possible case, compatible illness but no epidemiological link to confirmed case
What is significant exposure in this context? • EITHER 15 mins in same room as probable or confirmed case • OR face to face contact with probable or confirmed case • WITHIN 4/5 days before and 4 days after, rash appeared
School/Nursery Exclusion • Any child with Measles-like rash for 5 days after rash appeared • Any unvaccinated child with significant contact who develops symptoms suggestive of Measles prodrome • Unvaccinated siblings of probable/confirmed case
What constitutes vaccinated? • MMR vaccine failure is not rare, so MMRx2 needed to be confident that rash illness is not Measles
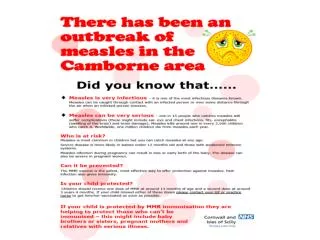
Measles in Camborne • Imported via family visit to London, unvaccinated child • Spread within school – rel low uptake area • Also to associated pre-school groups • Only 2 generations of spread
Joint working • Essential for DPH to be on board • Most important intervention is vaccinating around cases • Strategy was to start by encouraging GPs to vaccinate then to target schools affected, then those in the next ring outside
Vaccination strategy • Vaccination strategy was informed by availability of MMR cover data for children on school roll, enabled targeted approach to schools • Can also target schools with low uptake and pupils who are immunocompromised
Measles In Newquay • Case is adult teacher at secondary school • Waiting on results of 2 probable cases, 2 have already tested negative
Other case • Adult who had been to public venue in London ( War room) • Admitted to hospital • No other associated cases
What to learn from this? • Can’t be complacent about Measles with current MMR uptake levels and consequent population immunity • However, levels of immunity in SW are unlikely to support prolonged outbreaks, except where there are communities of low uptake individuals
Important preparations • Communications, ensure that public, primary care and secondary care know about the outbreak and what they need to do • Ensure that salivary kits are available in primary care – predistributed is best • Ensure that there is a system for obtaining HNIG promptly
Resources • Resources used in o/b to be combined into SW Measles pack through development group • Only problem, some represent draft documents not yet consulted on.
DRAFT Managing Individual Contacts of Measles. Chart 2 - for infants contacts of cases confirmed or where there is a high index of suspicion (note 1) IMPORTANT The table below applies to healthy infants. If there is a particular reason to avoid measles (such as a recent severe illness) obtain further advice. Note: If MMR is not given within 72 hours of exposure it may still be worthwhile as there may be further exposure at a later date (See note 4).
Yes No Is the contact pregnant? See note 3 and separate flow chart Yes No Likely to need HNIG as soon as possible but refer to ImmunoglobulinHandbook and seek advice from HPA or supervising hospital consultant. Is the contact immunosuppressed? (see note 2) Yes No • Has the contact: • Been fully vaccinated (2 doses of MMR) or • Had measles in the past (less likely to have had measles if born after 1970)? Advise vigilance for prodromal symptoms and investigate if symptoms develop Yes No See separate chart 2 Is the contact an infant aged 12 months or under Yes No Offer MMR as soon as possible (see note 4 AND Exclude from school, nursery, playgroup etc until beyond the incubation period or it is clear they don’t have measles or for the infectious period if become symptomatic. Is the contact an unvaccinated sibling of the case Yes No • Offer MMR as soon as possible (see note 4). Any dose should be at least a month after any previous dose. Is the contact unvaccinated or partially vaccinated? Yes
Does the pregnant contact have a well documented history of either 2 doses of MMR / measles vaccine? See Note 3 N Y Where time allows Serum should be taken for urgent measles specific IgG (where possible use antenatal booking specimens) Reassure as to low likelihood of infection If no time for IgG testing. i.e. result would not be available within 6 days of exposure Blood results: IgG detected within 10 days of contact with case? N Y Result received within 6 days of contact with case? N Y Probably immune – reassure as to low likelihood of infection Advise vigilance for prodromal symptoms and investigate if rash develops Offer HNIG as soon as possible. Take follow-up serum 3 weeks after contact with case Within 6 days of contact If antenatal serum not available collect and store serum. Advise vigilance for prodromal symptoms and investigate if rash develops Beyond 6 days of contact
Immunisation • It is relatively easy to target areas of low uptake successfully where this is due to access problems • However, dealing with parental refusal is much more difficult and long-term