Download
1 / 52
600 likes | 1.66k Views
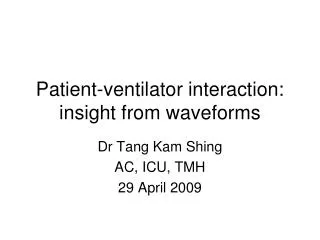
Patient-ventilator interaction: insight from waveforms. Dr Tang Kam Shing AC, ICU, TMH 29 April 2009. Waveforms on ventilators. Most modern ventilators have a graphical display on the panel of various mechanical parameters Mostly ignored in daily practices in ICU

E N D
Patient-ventilator interaction: insight from waveforms Dr Tang Kam Shing AC, ICU, TMH 29 April 2009
Waveforms on ventilators • Most modern ventilators have a graphical display on the panel of various mechanical parameters • Mostly ignored in daily practices in ICU • They actually give a lot of information regarding: • The mechanical properties of the respiratory system • The interaction between the patient and the ventilator
Waveforms on ventilators • However, there are several important points you have to bear in mind before you try to interpret waveforms • Whether the patient is paralyzed or actively breathing • The waveform analysis for both groups completely different • The mode of the ventilator is in • PCV or VCV (constant flow or decelerating flow)
Passive patients • Either paralysed or passive patients with no significant triggering or ventilatory efforts • General principle: • the controlled variable waveform usually showed not much information (because it is solely controlled by ventilator in passive patients) • The dependent variables waveforms showed much more information • For VCV, look at the pressure time and flow time waveform • For PCV, look at the flow time and volume time waveforms
Passive or paralyzed patient Volume control mode Constant flow
Constant flow (VC) • Idealized waveforms from constant flow volume control on left side • Real life tracing from ventilator
Pressure-time waveform • At the beginning of flow, an almost vertical pressure increase occurs • because of the frictional forces generated by gas flow • which is necessary to overcome the resistance of the airways and the ET tube • The curve shape then changes to a linear increase and follows a given slope to its maximum value • normally linear • Depends on the respiratory system compliance alone
Pressure-time in VCV • Upper tracing measures at ventilator • Lower tracing meaures at ET tube tip • 1st vertical part increased due to resistance of ET tube • 2nd part same due to identical compliance of respiratory system resistive compliance
Resistance problem Compliance problem
End-inspiratory pause hold • P2 is the static pressure of the respiratory system • Which in the absence of flow equals the alveolar pressure • reflects the elastic retraction of the entire respiratory system • pressure drop from PIP to P1 represents the pressure required to move the inspiratory flow along the airways • Representing the pressure dissipated by the flow-dependent resistances
End-inspiratory pause hold • slow post-occlusion decay from P1 to P2 depends on the viscoelastic properties of the system and on the pendulum-like movement of the air (pendelluft) • elastic rearrangement of lung volume • Allows the different pressures in alveoli at different time constants to equalize • Due to the inhomogeneity of the lung parenchyma • rapid zones (low time constant) emptied into slow zones (high time constant)
End-inspiratory pause hold • Cstat = VT/P2 • Cdyn = VT/PIP • static compliance of the respiratory system mirrors the elastic features of the respiratory system • dynamic compliance also includes the resistive (flow-dependent) component of the airways and the ET tube
Passive or paralyzed patient Pressure control mode
Pressure control ventilation • Salient points • Decelerating flow • Decelerating lung expansion • Constant pressure • Whether end-inspiratory pause occur depend on inspiatory time and mechanical properties of respiratory system
PIP and plateau pressures in PCV Flow stopped Plateau pressure
Resistance and compliance in PCV Increasing resistance Reducing compliance
Rate of pressurization in PCV Increasing rate of pressurization
Inspiratory artifacts common in daily practices Spike due to pressurization of circuit especially for low pressure rise time
Expiratory artifacts common in obstructive lungs COPD Spike from recoil of ventilator circiut Normal
Spontaneously breathing patients A bit more complicated
Patient-ventilator interaction • In passive patients • Basically only the ventilator and passive mechanical properties of respiratory system involved • Any abnormal pattern is due to the ventilator or the respiratory system • In actively breathing patients • 4 different systems interacting: ventilator, respiratory system, respiratory pump and central ventilatory drive • Patterns can be due to either one alone or in combinations
Now consider this… • There are two pumps with two control acting on the same respiratory system • Ventilator that is controlled by computer programs that is set by doctors (that commonly do not know what to do) • Neuro respiratory centre controlling the respiratory muscles with its own “desirable setting” (that commonly do not agree with doctors)
Patient-ventilator asynchrony • Simply means the two pumps are not agreeing with each other • A lot of times working against each other • Ineffective ventilation • Increase work of breathing prolonged weaning • I am simple minded, so in essence there are two ways to due with this problem • Stop the neuro drive if you believe the neuro drive is not appropriate by sedation +/- paralysis, may be needed in initial management of status asthmaticus • Change your ventilator setting to agree as much as possible with neuro ventilatory drive (best to do but not easy) • Change neuro drive to agree with your setting (impossible)
Types of asynchrony • Essentially 3 phases of mechanical ventilation can show asynchrony • Trigger asynchrony • Flow asynchrony • Termination (cycling) asynchrony
Trigger asynchrony • The ventilator failed to detect a patient trigger • Inspiratory effort completely wasted • The start of inspiration is slower or later than neural inspiration • Resulting in wasted efforts in the initial part of spontaneous breaths • Double triggering • Auto triggering
PEEP = 0 PEEP = 10 Failed trigger and PEEP setting
Other causes of auto-triggering • Too sensitive trigger setting • more prevalent in patients who had acquired valve disease and had more dynamic circulatory characteristics • Larger heart size • larger cardiac output • higher ventricular filling pressure • lower respiratory-system resistance). • result in larger cardiogenic pressure oscillations, which when transmitted to the airway, causing auto-triggering.
Pressure or flow trigger?? • 2 common types of trigger mechanism available on commercial ventilators: • pressure trigger and flow trigger • initial clinical studies indicated that flow-triggering offered some advantage in reducing trigger asynchrony • recent advances in the development of pressure transducers have resulted in nearly equivalent or comparable results
Flow asynchrony • Occurs whenever the ventilator flow does not match the patient flow requirement • a common problem, and the flow setting may be the most frequently incorrectly-set ventilator parameter • divided into 2 sections, based on the 2 general methods for delivering gas: • VCV with a fixed flow pattern • PCV with variable flow
Flow asynchrony in VCV • Remember the waveform of passive VCV breath with constant flow • The shaded area represent the work done by the respiratory pump of the patient
Flow asynchrony in PCV or PSV • In essence should not be inadequate flow as pressure is fixed with flow as required by patient • Still possible with too slow pressure rise time • In initial phase of respiration • Also result in a “dished out appearance in pressure waveform
Flow starvation from slow rise time 10% rise time 1% rise time
Too fast rise time flow asynchrony Pressure-time Flow-time
Cycling asynchrony • Basically two possibilities • Neuro expiration earlier than mechanical expiration, too late termination of support • Neuro expiration later than mechanical expiration, too early termination of support
Too late termination of support • Problem is we usually do not have EEG of expiratory muscles • Can we detect this problem with waveforms?
Too early cycling (cycling asynchrony) Notch in expiratory flow