Malaria: Factors, Control, and Development Impact
330 likes | 348 Views
Learn about the physical and human factors contributing to malaria risk, evaluate control strategies, and explore the benefits to developing countries. Understand how malaria impacts populations, economy, and health globally.

Malaria: Factors, Control, and Development Impact
E N D
Presentation Transcript
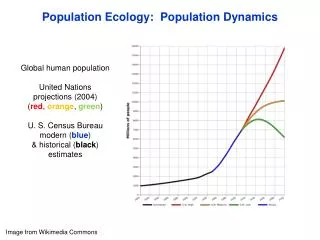
Higher Geography Population
Development & Health Malaria “describe the physical and human factors which put people at risk of contracting the disease
Development & Health Malaria “describe the physical and human factors which put people at risk of contracting the disease describe andevaluate thestrategies used in controlling the spread of the disease
Development & Health Malaria “describe the physical and human factors which put people at risk of contracting the disease describe and describe andevaluate the strategies used in controlling the spread of the disease explain the benefits to Developing Countries of controlling the disease.”
Development & Health Malaria Background - Malaria is a disease that affects over 100 countries in the world and kills 2.5 million people every year.
Development & Health Malaria
Development & Health Malaria “describe the physical and human factors which put people at risk of contracting the disease” It is caused by a tiny parasite entering the bloodstream and causes the victim to suffer from headaches and stomach pains, followed by fevers of high temperature and shivering fits. The fever can occur many times and frequently results in the victim’s death.
Development & Health Malaria Children are particularly vulnerable as they may not yet have been able to build up immunity from the disease. Even if it is not fatal, malaria can cause kidney failure and leaves the victim prone to catching other diseases. Life expectancy is considerably reduced. Malaria affects development economically too. A person’s productivity is seriously impaired (on farms or factories) and diverts some of that country’s government’s expenditure into caring for its victims. It causes high levels of absenteeism from work and can lead to areas of fertile farmland being abandoned – e.g. in northern Sri Lanka.
Development & Health Malaria The parasite that causes malaria is actually passed into the bloodstream by the female anopheles mosquito biting a victim, after it has already bitten an infected person. It feeds on the person’s blood but inadvertently passes on the parasite in its saliva. The mosquito is the carrier or vector, rather than its cause.
Development & Health Malaria Causes - Physical Physical causes of malaria Malaria occurs in areas populated by the anopheles mosquito (the vector is actually the female of the species). It needs stagnant or still water to be present as these are the breeding areas for the mosquitoes. And finally the temperatures must be relatively warm, over 16°C. Shaded areas, egtrees, buildings, also help as they allow digestion of blood meal by the mosquito.
Development & Health Malaria Causes - Human Human causes of malaria Malaria also needs certain human factors to contribute to its spread. People provide the blood that is consumed by the mosquito, so centres of populations are where you’ll find the mosquito - “blood reservoir” . Another major factor is poor sanitation and poor irrigation or drainage or dams as these provide the stagnant water needed. Other stagnant water sources to lay eggs include water tank wells, irrigation channels, water barrels and padi–fields The disease is also spread more now due to greater migration of people, including infected people, to different regions or countries.
Development & Health Malaria Methods of control - Cure “describe and evaluate the strategies used in controlling the spread of the disease” Methods of controlling malaria – attacking the parasite Malaria can be cured by drugs, such as the anti-malarial Chloroquin and quinine. However this is now less effective than in the past as the parasite have developed a resistance to these drugs. These methods are also relatively expensive, so many new methods now focus on attacking the vector, the anopheles mosquito, rather than the parasite.
Development & Health Malaria Methods of control - Prevention Eucalyptus trees Methods of controlling malaria – attacking the vector One approach is to remove stagnant pools of water in which the mosquito’s breed, so pools are drained and irrigation is made more efficient. Planting eucalyptus trees also helps here by absorbing moisture from the soil, reducing the chance of stagnant pools developing.
Development & Health Malaria Methods of control - Prevention The mosquito eggs can also be targeted. Water can be released from dams to drown the larvae or fish can be put into the water to eat them. The larvae can be suffocated by spraying egg white (albumen) on the surface of stagnant water. Mustards seeds can be used to drag the larvae below the water to drown them. Similarly drainage of stagnant water sources to eradicate breeding habitats but this is expensive technology and physically impractical.
Development & Health Malaria Methods of control - Prevention If the larva survives, then there are also methods of attacking the adult mosquitoes. Insecticides e.g. Malathion or DDT can be sprayed to kill them. However, as the WHO discovered, this may be successful initially but not in the long run. They ran a campaign in the 1950’s and 60’s in India and actually reduced malarial cases from 75 million to 1 million in 10 years. Unfortunately, the expense of the insecticides for a developing country, and the increasing resistance of the mosquitoes to the chemicals, reduced its effectiveness and water sources become polluted, damaging whole ecosystems.
Development & Health Malaria Methods of control - Prevention The figures have since risen to 2 million cases again. The WHO has tried to use other methods to attack the mosquito. Their scientists attempted to reduce mosquito populations by genetic engineering (introducing sterile male mosquitoes) into the ecosystem. To some extent this approach has been favoured over spraying with chemicals since the spraying can kill other forms of life and the water is also needed for other uses e.g. drinking, washing, crop irrigation and animal’s drinking water.
Development & Health Malaria Methods of control - Prevention Finally, another method to reduce malaria is by educating the people to reduce their chances of contracting the disease. Prevention is seen as being much more desirable than cure. Organisations like the Red Cross do this by taking someone from each village and training them in Primary Health Care (P.H.C.). The person then returns to the village and educates everyone else on health matters. This is suitable since it uses local people who are seen as being more acceptable to villagers and it is a relatively low-cost way of tackling the problem and is suited to local needs.. The sort of advice includes practical measures like persuading people to use mosquito bed nets, keeping skin covered with long sleeves and trousers, keeping lids on water containers, filling in puddles and reducing visits to the river or well.
Development & Health Malaria Success of methods How successful have these methods been in controlling malaria? Although there has been some progress in reducing malaria, it is obvious that these methods haven’t been completely successful in eradicating it since it still exists in large parts of the tropics. Malaria is endemic over an area affecting more people in 2003 than it was in 1975. The WHO now accepts that total eradication is unlikely, and this is hardly surprising when we compare the £40 million spent on researching malarial cures to the £600 million currently being spent on Aids. The strategy now is for control.
Development & Health Malaria Success of methods As we have already seen, the use of insecticides, while initially effective, has become less so as the mosquitoes and parasites have become immune to the chemicals. We have actually witnessed recent increases in malaria in some places due to this e.g. in Sri Lanka. More than 400 million people now suffer from the disease worldwide, and no total vaccination (a drug that will prevent a person from contracting the disease if bitten) hasn’t yet been developed. The problem is exacerbated by the construction of large scale irrigation and dam schemes that can provide the stagnant water for the mosquitoes to breed in.
Development & Health Malaria Success of methods It should also be remembered that using chemical sprays has problems for other plants and water users, whilst attempts to drain stagnant water pools can never be completely effective since new ‘puddles’ can occur at any time e.g. a pothole in the road, and to totally drain an entire area in a wet climate would be extremely expensive, particularly for a poorer developing country.
Development & Health Malaria Success of methods The use of anti malarial drugs by people also shows an increasing level of resistance as well as having unpleasant side effects. Genetic engineering may well offer great hope in the future but there is also concern over using new, untested and ethically questionable techniques.
Development & Health Malaria Success of methods It is not all gloom. There have been many successes (within the Middle East, parts of N Africa and parts of South and SE Asia). Over 500 million people have been freed from endemic malaria. The problem is that population growth has been so great in other areas that in total, more people are in danger zones. Fewer people are actually dying from the effects of malaria now than 50 years ago. Undoubtedly there is an increased awareness by the local people and they generally take all reasonable precautions. Organisations such as the Red Cross are active in providing drugs, equipment and trained people for endemic areas. However the early success in areas such as India in the 1950s have not been maintained. Why? First, programmes are very expensive and cannot always be maintained. When compared with AIDS research, malarial eradication programmes only attract 10% of AIDS funding. Look again at the variety of prevention and control methods. Draining breeding grounds and spraying insecticides is expensive, requires lots of human labour and needs to be organised.
Development & Health Malaria Benefits of control “explain the benefits to Developing Countries of controlling the disease.” What are the benefits of controlling malaria? Despite the fact that controlling malaria is proving very difficult, if not impossible, and incredibly expensive, the countries affected still see the need to at least attempt to reduce it. Firstly, if they do manage to reduce the numbers of people affected by malaria it will save huge amounts of money on health, medicine and doctors, and then this money could be used elsewhere to improve people’s quality of life eg sanitation, water supplies, education etc. The people will then be fitter (less absenteeism) and more able to be more productive in the economy, either growing crops or in factories. They will produce wealth for the country whilst be able to spend their greater incomes helping their local economy.
Development & Health Malaria Benefits of control By producing more they will also address problems of a trade deficit, by having to import less and by exporting more. This in turn reduces the amount the government has to borrow i.e. national debt. The country will also receive a boost in its income from tourists as the threat of catching the disease may put some people off visiting the country. Finally if progress is made in eradicating malaria it will reduce damage caused to landscape and ecosystems by spraying and draining areas. These areas can once again become productive, extending the land under cultivation or giving more room for settlement or industry
Development & Health Malaria Primary Health Care The system of Primary Health Care is an extremely appropriate method of improving access to good health in developing countries. It is a system that uses local people to diagnose and treat local health problems. Villagers feel less intimidated going to a familiar face in more comfortable surroundings of their own area, rather than going miles to be examined by a stranger.
Development & Health Malaria This in itself could make it more useful as people are more likely to use such a service, rather than “suffering in silence” by not going to seek medical help elsewhere. It is an inexpensive way to provide poor areas with medical help, as the people who treat patients need not be fully trained medics – they may only be able to help a few crucial ailments their fellow villagers routinely suffer from. It also employs local methods to treat problems and so are less reliant on outside help – encouraging a ‘self-help’ attitude amongst the people.
Development & Health Malaria The types of activities that go to make up a Primary Health Care System include some of the following. As already mentioned local residents are used as paramedics or ‘barefoot doctors’. They have the advantage of being trusted by locals and are relatively cheap to train. This means that a lot of these people can be trained, often supported by a network of ‘trained helpers’ who can be referred to if the paramedics can’t fully deal with the problem. Treatment usually comes from locally produced medicines which are cheaper and more readily available than expensive drug from Western pharmaceutical companies – currently a major drug company is contesting the legality of this approach through international courts!
Development & Health Malaria Health education is another facet of the P.H.C. programme, again trying to prevent rather than cure. These can be focused on certain high risk groups e.g. children or expectant mothers, and often addresses personal and social habits that may contribute to better health in the future. Such education programmes are typical in poor urban areas in developing countries.
Development & Health Malaria The system has the flexibility to offer procedures to patients that neither the ‘barefoot doctors’ nor the ‘trained helpers’ can deal with, if they can travel to purpose built medical centres. Although further from the patient, it does offer more specialist treatment from the equivalent of a G.P. in the U.K
Development & Health Malaria In a more practical sense, certain treatments are common in a P.H.C. scheme. Oral Rehydration Therapy (O.R.T.) treats dehydration and diarrhoea problems and is cheap and easy to administer.
Development & Health Malaria A major element in P.H.C. is the provision of clean water since 80% of diseases in the developing world are caused by dirty water. Education programmes take place to encourage the use of better hygiene practices. Water can be purified with the use of special tablets that remove any harmful bacteria. The use of deep water wells, the location of which can be decided in part by the villagers, uses relatively cheap technology which is easy to use and maintain. Ensuring that water supplies are kept covered to reduce the opportunity for contamination e.g. by mosquitoes breeding in them. Areas of infected water can be improved with spraying or chemical cleansing.
Development & Health Malaria Model answer 1 Give examples of Primary Health Care strategies and comment on their effectiveness in improving health and controlling disease in areas you have studied. (6 marks) PHC aims to make good health care available to all the people in a country. In Nicaragua,the introduction of local health clinics saw a drop in infant mortality (from 30% to 8%). Mass vaccination eradicated polio and reduced the incidence of whooping cough, and malaria has almost been eliminated. In general, PHC programmes establish health clinics, encourage sanitation and clean water projects. They encourage local village dispensaries using traditional medicines. The use of 'barefoot doctors', supported by trained helpers can treat over 80% of most illnesses and ill health. Health education projects are linked to local mothers' groups and schools. Local clinics are linked to a referral structure whereby most complex cases can be moved to specialists. In general, these programmes have been very successful. They involve local people who are known and can be trusted. They are most effective in rural areas that are often remote and isolated, with limited existing educational and medical support. However too few health workers have been trained to meet the needs of the most troubled communities. There always remains a lack of funding and a lack of volunteers. The early successes have been hit by war, economic depression and natural disasters such as famine or earthquake. Undoubtedly there is an increased awareness by the local people and they generally take all reasonable precautions. Organisations such as the Red Cross are active in providing drugs, equipment and trained people for endemic areas. However the early success in areas such as India in the 1950s have not been maintained. Why? First, programmes are very expensive and cannot always be maintained. When compared with AIDS research, malarial eradication programmes only attract 10% of AIDS funding. Look again at the variety of prevention and control methods. Draining breeding grounds and spraying insecticides is expensive, requires lots of human labour and needs to be organised.
Development & Health Malaria Undoubtedly there is an increased awareness by the local people and they generally take all reasonable precautions. Organisations such as the Red Cross are active in providing drugs, equipment and trained people for endemic areas. However the early success in areas such as India in the 1950s have not been maintained. Why? First, programmes are very expensive and cannot always be maintained. When compared with AIDS research, malarial eradication programmes only attract 10% of AIDS funding. Look again at the variety of prevention and control methods. Draining breeding grounds and spraying insecticides is expensive, requires lots of human labour and needs to be organised. http://www.expresshealthcaremgmt.com/20050831/ruralhealthcare01.shtml http://www.earthinstitute.columbia.edu/cgsd/documents/bajpai_primaryhealth.pdf http://en.wikipedia.org/wiki/Healthcare_in_India