Download
1 / 35
350 likes | 427 Views
Understand the mechanism and effects of adrenergic agonists and antagonists, including therapeutic uses, adverse effects, and pharmacological actions. Learn about catecholamines, direct-acting agonists, and receptor antagonists.

E N D
Adrenergic agonists and antagonists Hashem Mansour
THE ADRENERGIC NEURON • Adrenergic neurons release norepinephrine as the primary neurotransmitter. • These neurons are found in the central nervous system (CNS) and in the sympathetic nervous system. • Drugs that activate adrenergic receptors are termed sympathomimetics.
Adrenergic receptors (adrenoceptors) • The receptors are divided into two groups alpha (α) and beta (β) receptors. • These are further subdivided to α1, α2, β1 and β2 • This depend on the responses to epinephrine, norepinephrine, and isoproterenol
Mechanism of action of adrenergic agonists (sympathomimetics) • Direct : epinephrin • Indirect : cocain • Mixed : pseudoephedrin
ADRENERGIC AGONISTS • A. Catecholamines: such as epinephrine, norepinephrine, and dopamine • B. Noncatecholamines: phenylephrine, ephedrine .
DIRECT-ACTING ADRENERGIC AGONISTS epinephrin and Norepinephrine • Epinephrine • At low doses, β effects (vasodilation) on the vascular system predominate, whereas at high doses, α effects (vasoconstriction) are the strongest. • 1. Actions: • a. Cardiovascular: positive inotrope and chronotropic effect • Kidney cause renin release. increase systolic blood pressure.
DIRECT-ACTING ADRENERGIC AGONISTS epinephrin andNorepinephrine • Respiratory: bronchodilation. • Hyperglycemia: Epinephrine has a significant hyperglycemic effect because of increased glycogenolysis in the liver and decrease insulin release. • Lipolysis: Epinephrine initiates lipolysis.
Adverse effects • Restlessness, palpitation, anxiety, tremor. • Rise in BP leading to cerebral hemorrhage, ventricular tachycardia/fibrillation, angina, myocardial infarction.
Contra indication • Adrenalin is contraindicated in hypertensive, hyperthyroid and angina patients. • Adrenalin should be used very cautiously in patients with heart disease. • It should not be given to patients receiving β blockers (marked rise in BP can occur).
Oxymetazoline • Over-the-counter short-term nasal spray decongestants, as well as in ophthalmic drops. • Rebound congestion and dependence are observed with long-term use.
Albuterol and terbutaline • Albuterol is the β2 agonist of choice for the management of acute asthma symptoms. • Side effects: tremor, restlessness, and anxiety, tachycardia or arrhythmia especially in patients with underlying cardiac disease.
THERAPEUTIC USES • Hypotensive states (shock NA) • Adrenalin is the drug of choice for anaphylactic life-saving. • Control of local bleeding from skin, mucous membranes, tooth socket, epistaxis
Therapeutic uses • Nasal decongestant In colds, rhinitis, sinusitis • Cardiac arrest • Bronchial asthma. • Uterine relaxant used to postpone (prevent premature) labour.
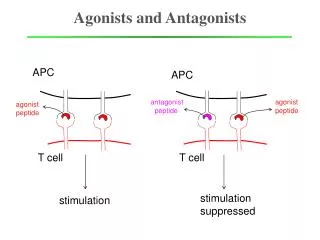
ADRENERGIC RECEPTOR ANTAGONISTS • These are drugs which antagonize the receptor action of adrenaline and related drugs.
α ADRENERGIC BLOCKING DRUGS • Phenoxybenzamine, Chlorpromazine, Prazosin, Tamsulosin, Alfuzosin.
GENERAL EFFECTS OF α BLOCKERS • Reduces peripheral resistance and cardiac output → fall in BP. • Nasal stuffiness and miosis. • Intestinal motility is increased • Reduce renal blood flow → increase in blood volume. • Tone of smooth muscle in bladder trigone, sphincter and prostate is reduced → urine flow in patients with benign hypertrophy of prostate (BHP) is improved.
USES OF α BLOCKERS • Hypertension :Prazosin is primarily used as an antihypertensive. • Pheochromocytoma • Benign hypertrophy of prostate (BHP) doxazosin and tamsulosin • Raynaud’s phenomenon: symptomatic relief when vasoconstriction is prominent
β ADRENERGIC BLOCKING DRUGS • CLASSIFICATION • Nonselective (β1 and β2)Propranolol, Labetalol, Carvedilol. • Cardioselective (β1) Atenolol, Bisoprolol.
PHARMACOLOGICAL ACTIONS • 1. Heart decreases heart rate, force of contraction and output (c.o.). • 2. Blood vessels: vasodilatation • 3. Respiratory tract Increases bronchial resistance . • 4. Metabolic Increase in plasma free fatty acid levels. It also inhibits glycogenolysis • 5. Eye Reduces secretion of aqueous humor: i.o.t. is lowered.
ADVERSE EFFECTS AND CONTRAINDICATIONS • Bradycardia, worsen CHF. • Can precipitate life-threatening attack of bronchial asthma: contraindicated in asthmatics. • Worsening of angina and even sudden death can occur. • Propranolol is contraindicated in partial and complete heart block: arrest may occur. • Sleep disturbances, nightmares.
Cardioselectiveβ1BLOCKERS • Atenolol and bisoprolol. • More selective in blocking (β1) than (β2) receptors. • Have lower propensity (tendency) to cause bronchoconstriction. • Bradycardia and depression of contractility at rest are not prominent.
Uses of beta blockers • Timolol:used topically in the eye for glaucoma. • Hypertension: β blockers for mild antihypertensives. • Angina pectoris selective beta blockers benefit angina of effort • Cardiac arrhythmias: β blockers suppress tachycardias.
Uses of beta blockers • Secondary prophylaxis of MI: bisoprolol • Congestive heart failure: bisoprolol. • Thyrotoxicosis: Propranolol rapidly controls symptoms. • Migraine Propranolol is the most effective drug for chronic prophylaxis of migraine
α + β ADRENERGIC BLOCKERS • Labetalol It is the first adrenergic antagonist capable of blocking both α and β receptors. • Used in treatment of emergency hypertension
Impact in physiotherapy • Sympathomimetic drugs are prescribed in the treatment of upper and lower respiratory dysfunctions • Sympatholytic drugs are prescribed in the treatment of various cardiovascular disorders
CLINICAL RELEVANCE FOR REHABILITATION • Adverse Drug Reactions • Central nervous system: restlessness and insomnia. • Alpha agonists may increase blood pressure and precipitate angina pectoris in patients during aerobic rehabilitation activities. • Beta2 agonists may increase heart rate and precipitate angina pectoris or cardiac dysrhythmias. • Orthostatic hypotension is a problem with many of the sympatholytic drugs. • Bronchoconstriction is a problem with the β-receptor antagonists.
Effects Interfering with Rehabilitation • Orthostatic hypotension may cause patients to faint when transferring from sitting or supine positions to standing, exiting from a warm aqua therapy area, or if aerobic exercise is terminated without an appropriate cool-down period. • Dyspnea may decrease the aerobic capacity of patients.
Possible Therapy Solutions • To prevent fainting associated with orthostatic hypotension, assist patients with positional changes and when exiting a warm pool. • Always provide a cool-d own period following a period of exercise. • Allow increased time to complete aerobic tasks to prevent dyspnea and account for depressed cardiac activity.
Possible Therapy Solutions • Check blood pressure and heart rate prior to and following aerobic activities. • Monitor heart rate during aerobic activities. • Potentiation of Functional Outcomes Secondary to Drug Therapy • Patients with asthma or other respiratory dysfunction may benefit from the use of β2 agonists prior to aerobic activities..