Download
1 / 29
300 likes | 962 Views
Cholinergic agonists & Cholinergic antagonists Adrenergic agonists & Adrenergic antagonists. Part I. Cholinergic agonists. 1. direct cholinergic agonists 2. cholinesterase inhibitors .

E N D
Cholinergic agonists & Cholinergic antagonists Adrenergic agonists & Adrenergic antagonists
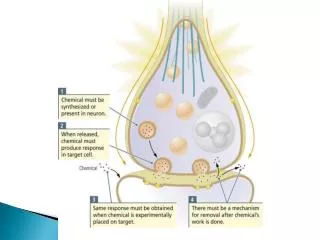
Part I.Cholinergic agonists 1.direct cholinergic agonists 2.cholinesterase inhibitors. two main targets of drug action: the postsynaptic receptor and the acetylcholinesterase enzyme, which breaks down acetylcholine. direct-acting cholinergic agonists have a direct action on the receptor for acetylcholine. Some drugs are specific for the muscarinic receptor; others are specific for the nicotinic receptor
The indirect-acting cholinomimetics act by blocking the metabolism of acetylcholine by cholinesterases. These drugs effectively increase the concentration of acetylcholine at all cholinergic synapses. The enzyme that is specific for acetylcholine is called acetylcholinesterase, and it is found on both the pre- and postsynaptic membranes.
There are other cholinesterases that also metabolize acetylcholine and drugs with related structures. These other cholinesterases are sometimes called pseudocholinesterases or nonspecific cholinesterases, and they are abundant in the liver.
Direct cholinergic agonists 1. esters: - structurally related to acetylcholine, e.g. bethanechol (used in the treatment of urinary retention) 2. alkaloids: pilocarpine; muscarine The effects of all of these agents are exclusive muscarinic. side effects often listed for these drugs include sweating (increased secretion), salivation, GI distress, and cramps (due to increased motility).
Effects of Autonomic Nerves Activity on Organ Function parasympathetic organ sympathetic
nicotine is a direct agonist at nicotinic receptors. nicotine is used therapeutically to help patients stop smoking.
Cholinesterase inhibitors Reversible (water soluble e.g. Physostigmine, Neostigmine) and irreversible inhibitors (lipid soluble e.g. organophosphates) The reversible inhibitors include the quaternary amines and the carbamates. They compete with acetylcholine for the active site on the cholinesterase enzyme. This group includes the drugs with names ending in "-stigmine" and "-nium." The irreversible inhibitors phosphorylate the enzyme and inactivate it. These cholinesterase inhibitors are widely used as insecticides e.g.: Parathion and are commonly referred to as nerve gases e.g.Sarin . Because the organophosphates are lipid soluble, they rapidly cross all membranes, including skin and the blood-brain barrier.
Pralidoxime (2-PAM) and Atropine are used to treat poisoning with organophosphates
These drugs [reversible cholinestrease inhibitors] have all the same actions (and side effects) as the direct acting drugs (muscarinic). In addition, because they increase the concentration of acetylcholine, they have effects at the neuromuscular junction (nicotinic). These drugs will cause the same side effects as the direct cholinergic agonists. They also affect nicotinic receptors, primarily at the neuromuscular junction. This is the basis of their therapeutic use. They cause fasciculations and weakness in normal people and can improve muscle strength in patients with myasthenia gravis. Myasthenia gravis is an immune disease in which there is loss of acetylcholine receptors at the neuromuscular junction, resulting in weakness and fatigability of skeletal muscle.
These drugs [reversible cholinestrease inhibitors] can have effects on the cholinergic system in the CNS, if the drug can cross the blood-brain barrier. The effects range from tremor, anxiety, and restlessness to coma. The organophosphates, because of their lipid solubility, rapidly cross into the CNS. Neostigmine, Pyridostigmine are used in the treatment of myasthenia gravis. Other uses of the reversible cholinesterase inhibitors are in the treatment of open-angle glaucoma and the reversal of nondepolarizing neuromuscular blockade after surgery (e.g. tubocurarine but not succinylcholine).
Part II. Cholinergic antagonists The prototypic muscarinic antagonist is Atropine. All of the muscarinic antagonists are competitive antagonists for the binding of acetylcholine to the muscarinic receptor. Muscarinic antagonists are used preoperatively to reduce secretions. [although sweating glands are enervated by sympathetic nerves, ACh is the neurotransmitter and the receptors is muscarinic.]
Scopolamine (also called hyoscine) is used to prevent motion sickness. Muscarinic antagonists e.g. oxybutynin are used for urinary frequency, urgency caused by bladder overactivity.
Ganglionic blockers: they block the action of Ach at the nicotinic receptor of all autonomic ganglia. These drugs are very rarely used clinically.
Neuromuscular blockers: The competitive neuromuscular blocking drugs are used to produce skeletal muscle relaxation. Succinylcholine is a depolarizing neuromuscular blocker. Botulinum toxin blocks the release of acetylcholine at all cholinergic synapses. Tubocurarine: is among the drugs thatcompete with acetylcholine for the receptor but do not initiate ion channel opening.
Part III. Adrenergic agonists Direct-acting Agonists Epinephrine has a number of uses, including the treatment of allergic reactions and shock. The control of localized bleeding and the prolongation of the action of local anesthetics. Norepinephrine has a relatively low affinity for b2 receptors. The main effect of al stimulation (with an agonist such as phenylephrine) is vasoconstriction. Local application of a vasoconstrictor to the nasal passages decreases blood flow locally and decreases secretions, thus acting as a nasal decongestant.
Dopamine- at low doses, Dopamine causes renal and coronary vasodilation. At high doses, dopamine acts much like epinephrine. It also activates b1 receptors in the heart.
Indirect-acting Agents The indirect-acting sympathomimetic agents act by releasing previously stored norepinephrine. Amphetamine and its relative, methylphenidate, are central nervous ,stem stimulants used to treat attention deficit hyperactivity disorder in children. Amphetamine and others of its relatives are indirect-acting sympathomimetics that have been abused because of their psychostimulant abilities. Norepinephrine increases total peripheral resistance and mean arterial pressure. Epinephrine predominantly affects the heart through b1 receptors, causing an increase in heart rate and cardiac output. Isoproterenol causes a marked decrease in total peripheral resistance and n increase in heart rate and cardiac output.
Part IV. Adrenergic antagonists a2 Agonists reduce sympathetic nerve activity and are used to treat hypertension. (clonidine) a BLOCKERS most of the a antagonists allow vasodilation and thus, decrease blood pressure. The side effects of the a -blockers are directly related to their a Blocking activity. All of` the a blockers are reversible inhibitors of the a receptor. except pheoxybenzamine, which is irreversible.
b-BLOCKERS- the b -blockers have widespread use in the management of cardiac arrhythmias, angina, and hypertension.e.g. propranolol b1 Selective antagonists are often referred to as cardioselective e.g. acebutolol. b2 anatgonists causes contraction of smooth muscle- dangerous to asthma patients The adverse effects of these drugs are, for the most part, directly related to their b blocking abilities. Some b -blockers are said to have intrinsic sympathomimetic activity. This means they have partial agonist activity, even though they are classified as b -blockers.