Download
1 / 120
1.21k likes | 1.39k Views
Comprehensive guide for diagnosing neurological levels, muscle power, and reflexes. Explore nerve root lesions, sensory evaluation, and upper extremity muscle testing. Visualize muscle grading, sensation, and reflex patterns.

E N D
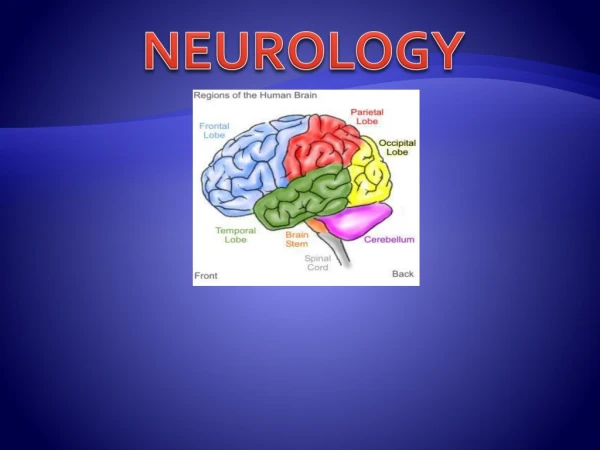
Orthopaedic Neurology Diagnostic Guide to Neurological Levels
Motor Power • Interruption of the nerve root causes denervation and paralysis of its myotome. • Pressure on a nerve root can cause a decrease in muscle strength. • Muscle testing is utilized to evaluate whether or not a lesion is present and to what degree it is effecting the muscle strength.
Muscle Grading Chart • Muscle gradations • 5 – normal • 4 – good • 3 – fair • 2 – poor • 1 – trace • 0 - zero • Description. • Complete range of motion against gravity with full resistance. • Complete range of motion against gravity with some resistance. • Complete range of motion against gravity. • Complete range of motion with gravity eliminated. • Evidence of slight contractility. No joint motion. • No evidence of contractility.
Sensation • Pathology to the cord or nerve root results in loss of light touch, followed by loss of sensation of pain. • During recovery from nerve root injury, sensation of pain returns before light touch.
Sensation • The 2 sensations are tested separately, light touch with a cotton swab, pain with pinpricks. • Pinwheels can be utilized to evaluate sensation. • Results can be recorded on a dermatome chart as normal, hyperesthetic (increased), hypoesthetic (decreased), dyesthetic (altered), or anesthetic (absent).
Reflex • Interruption in the basic reflex arc results in the loss of reflex, while pressures on the nerve root itself may decrease its intensity (hyporeflexia). • Interruption of the upper motor neuron’s regulatory control results in a hyperactive nerve (hyperreflexia). • Reflexes should be reported as normal, increased, or decreased utilizing bilateral comparison.
Evaluation of Nerve Root Lesions Upper Extremity
Cervical Spine • C5 is the 1st significant contribution to the brachial plexus. • C1-4 are difficult to test; However, C4 is the major innervation to the diaphragm (via the phrenic nerve).
Extensor Carpi Ulnaris (Left), Extensor Carpi Radialis (Right)
Flexor Digitorum Superficialis (Left), and Profundus (Right)