Neurology
Neurology. The Skull. The brain’s protector. The Skull. Made of 8 irregularly fused bones. Smooth on the outside, folds and ridges on the inner surface. The Cranial Vault. Foramen magnum. The Brain (80%). Increased Brain Volume. Mass. Cerebral Swelling.


Neurology
E N D
Presentation Transcript
The Skull The brain’s protector
The Skull Made of 8 irregularly fused bones Smooth on the outside, folds and ridges on the inner surface
Increased Brain Volume • Mass • Cerebral Swelling
Normally about 750cc of circulating volume 20% of the Cardiac Output Blood (10%)
Increased Blood Volume • Hemorrhage • Vasodilatation
Increased CSF Volume • Hydrocephalus
Intracranial Pressure (ICP) • The pressure exerted by the brain tissue, intracranial blood, & CSF
Dura Mater Tough Mother
Double layered Inelastic, fibrous membrane Holds the brain in place Dura Mater
Epidural Space • Space that is directly above the Dura • Middle Meningeal Artery is present here
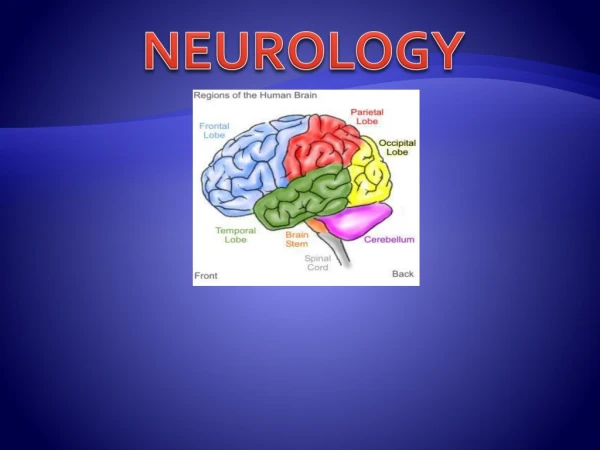
Frontal lobe Impulses Movement
Frontal lobe Personality Spoken Language
Parietal lobe Touch Understanding Sight Understanding
Parietal lobe Distance and Position to Objects
Temporal lobe Hearing Written Words Memory
Brainstem Pons Mid Brain Medulla Oblongata
Down and Dirty • ABC’s First • Quick History • LOC • Vital Signs • Pupils • Early or Late? • Early: restlessness, disorientation, lethargy • Late: Increase BP, pupillary changes, seizures
Assessment • GLASGOW COMA SCALE • Best Eye Opening • Best Verbal Response • Best Motor Response
Best Eye Opening • Spontaneously-4 • To Verbal Command-3 • To Pain-2 • No Response-1
Best Verbal Response • Oriented, Converses-5 • Disoriented, Converses-4 • Inappropriate words-3 • Incomprehensible sounds-2 • No Response-1
Best Motor Response • Obeys Commands-6 • To Pain • Localizes Pain-5 • Flexion Withdrawal-4 • Abnormal Flexion-3 • Abnormal Extension-2 • No Response-1
Glasgow Coma Scale Pediatrics • Verbal (2 to 5 years) • Appropriate words or -5 • Inappropriate words-4 • Persistent cries and/or screams-3
Glasgow Coma Scale Pediatrics • Verbal (0 to 23 months) • Smiles or coos appropriately-5 • Cries and consolable-4 • Persistent inappropriate crying and / or screaming-3
Severity of Injury • Mild • GCS Score 14-15 • Moderate • GSC Score 9-13 • Severe • GCS Score 3-8
Loss of Consciousness“A,E,I,O,U TIPS” • A • Alcohol • E • Epilepsy • I • Insulin (too much, too little) • O • Oxygen (too much, too little) • U • Uremia or other metabolic issues • T • Trauma, toxicity, tumors, thermoregulation • I • Infections, ischemia • P • Psychiatric, poisonings • S • Stroke, syncope or other neurologic / cardiovascular causes
Babinski’s Reflex • Present when stroking of Planter surface of foot causes • Flexing of great toe • Fanning of other toes • Normally present in children <2yo • Presence in >2yo indicates problem in corticospinal tract (nerve path spine to brain)
Abnormal posturing is a late sign of increasing ICP Decorticate Abnormal flexion Decerebrate Abnormal extension
Meningeal Signs • Nuchal rigidity • Stiff neck, pain on flexion • Photophobia • Positive Brudzinski’s • Involuntary flexion of knees/hips when neck flexed • Positive Kernig’s • Unable to straighten leg when hip fully flexed in supine patient
Intracranial Pressure • Intracranial pressure reflects • Brain • Cerebrospinal fluid • Blood • As intracranial pressure increases, cerebral perfusion pressure decreases • Leads to cerebral ischemia and hypoxia • In a hypotensive patient, even a marginally elevated ICP can be harmful • Adequacy of cerebral perfusion pressure is most important
Increased Intracranial Pressure • Initially -intracranial volume increases-ICP remains stable. • System becomes less compliant, or less able to tolerate increases in volume • Later, intracranial volume cont’s to increase, less compliance will be unable to buffer the increases and ICP will rise
Increased Intracranial Pressure Assessment • Early picture of increased intracranial pressure (IICP) • LOC • Loss of insight • Loss of recent memory • Restless, irritable, uncooperative behavior • Requires more stimulation to get same response • Speech less distinct • Sudden quietness in a very restless patient
Increased Intracranial Pressure Early Increasing ICP Motor function • Usually contralateral to lesion • Pronator drift • Loss of one or more grades on the strength scale • Increased tone
Increased Intracranial Pressure • Early Increasing ICP • Pupils • Sluggish to light response • Usually unilateral • Ipsilateral to lesion • Papilledema or bulging of optic discs • Blurred vision
Increased Intracranial Pressure • Early Increasing ICP • Vital signs • Occasionally tachycardic • Occasional hypertensive swings
Increased Intracranial Pressure • Late Increasing ICP • LOC • Arousable only with deep pain • Unarousable • Motor function • Dense hemiparesis • Abnormal flexion • Abnormal extension • No response (flaccidity preliminary to death)