Download
1 / 115
1.16k likes | 1.5k Views
HANDOUT OF LEARNING GASTROINTESTINAL SYSTEM. By Ni Ketut Alit A Faculty Of Nursing Airlangga University. Function of G I system. The Primary Digestive Functions are Break down food particles “molecular forms” Absorb into the bloodstream the small molecules

E N D
HANDOUT OF LEARNINGGASTROINTESTINAL SYSTEM By Ni Ketut Alit A Faculty Of Nursing Airlangga University
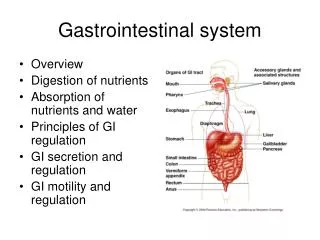
Function of G I system • The Primary Digestive Functions are • Break down food particles “molecular forms” • Absorb into the bloodstream the small molecules • Eliminate waste products & undigested food
Function of G I system • Chewing & Swallowing • 1.5 L of saliva are secreted daily • Ptyalin “salivary amylase” starch digestion • Saliva lubricate food as it chewed & swallowed • Gastric function • Hydrochloric acid to destruct most ingest bacteria ,& break down food • Pepsin for initiation of protein digestion • Intrinsic factors • The food mixed with gastric secretions is called chyme
Function of G I system • Small Intestine function • Pancreas : -Trypsin aids in digestion of proteins -Amylase aids in digestion starch -Lipase aids in digestion of fats • Liver : bile aids in emulsifying ingested fats • Intestinal Glands :secrete mucus ,hormones ,electrolytes ,and enzymes • Two types of contractions • Segmentation contraction • Intestinal peristalsis
Function of G I system • Colonic Function • Two types of colonic secretion -Mucus: protect colonic mucosa -Electrolytes: mainly “HCo3” neutralize the end products • Slow peristaltic to allow absorption of water & electrolytes
Assessment • Health history ( diet history ,appetite , weight gain & loss , stool ch.ch.,& eating pattern • Clinical Manifestations :- • Pain • Indigestion • Intestinal Gas • Nausea & Vomiting • Change in Bowel Habits &Stool ch.ch.
Assessment • Physical Assessment • Inspection • Auscultation • Palpation • Percussion
Assessment • Diagnostic Evaluation • Upper GI tract study • Lower GI tract study • Gastric Analysis • Endoscopy • Laparoscopy (Peritoneoscopy ) • Anoscopy ,proctoscopy ,&Sigmoidscopy • Colonoscopy • Abdominal U/S , Abd CT scan ,&Abd MRI
Assessment • Stool Tests -Analysis & culture -occult blood test • Hydrogen Breath Test • Urea Breath Test • Tagged Red Blood Cells & Leukocytes
Disorders of the Jaw • Abnormal conditions affecting the mandible (Jaw)& the tempomandibular joint include congenital malformation, fractures , chronic dislocation , cancer , & syndrome ch.ch pain & limited motion • Tempomandibular Disorders Are a group of conditions that cause pain &\or dysfunction of the tempomandibular joint &/or the muscle of mastication, as well as contiguous tissue components
Disorders of the Jaw • Clinical Manifestations • Pain (from dull to throbbing ) • Debilitating pain radiated to the ears, teeth, neck muscle & facial sinuses • Restricted jaw motion & clicking • Difficulty chewing & swallowing • Depression may accompany
Disorders of the Jaw • Management • Patient education in stress Management • Range of motion exercises • Pain Management (NSAID) • Muscle relaxant &/or mild antidepressant
Parotitis • Inflammation of the parotid gland is the most common inflammatory condition of the salivary gland • Mumps (epidemic Parotitis) viral seen in children • Clinical Manifestations • Fever & red shiny skin • The gland swells ,tense ,&tender • Pain felt in ear • Swollen gland interfere with swallowing
Parotitis • Medical Management • Preventive Measures (dental care, oral hygiene, adequate fluid& nutrition ,& D/C of medication that may diminished salivary secretion) • Antibiotics for infection • Analgesic for pain • Drainage of gland • Parotidectomy
Impaired Esophageal Motility Achalasia • Achalasia: characterized by impaired peristalsis of smooth muscle of esophagus and impaired relaxation of lower esophageal sphincter • Manifestations: • Dysphagia • chest pain (pyrosis) • Sensation of food stick in lower esophagus • Food regurgitation
Achalasia Treatment • Eat slowly &drink fluids with meals • Calcium channel blockers • Endoscopically guided injection of botulinum toxin • Balloon dilation of lower esophageal sphincter or pneumatic dilation • Esophageal myotomy (abdominal or thoracic approach
Gastroesophageal Reflux Disease (GERD) 1. Definition • GERD common, affecting 15 – 20% of adults • Because of location near other organs symptoms may mimic other illnesses including heart problems • Gastroesophageal reflux is the backward flow of gastric content into the esophagus.
Gastroesophageal Reflux Disease (GERD) 2. Pathophysiology • a. Gastroesophageal reflux results from transient relaxation or incompetence of lower esophageal sphincter, sphincter, or increased pressure within stomach • b. Factors contributing to Gastroesophageal reflux 1.Increased gastric volume (post meals) 2.Position pushing gastric contents close to Gastroesophageal juncture (such as bending or lying down) 3.Increased gastric pressure (obesity or tight clothing) 4.Hiatal hernia
Gastroesophageal Reflux Disease (GERD) Manifestations • Heartburn after meals, while bending over, or recumbent • Dyspepsia or indigestion • May have regurgitation of sour materials in mouth, pain with swallowing • Atypical chest pain • Sore throat with hoarseness
Gastroesophageal Reflux Disease (GERD) 6. Diagnostic Tests • a. Barium swallow (evaluation of esophagus, stomach, small intestine) • b. Upper endoscopy: direct visualization; biopsies may be done • c. 24-hour ambulatory pH monitoring
Gastroesophageal Reflux Disease (GERD) 7. Medications • a. Antacids for mild to moderate symptoms, e.g. Maalox, Mylanta, Gaviscon • b. H2-receptor blockers: decrease acid production; given BID or more often, e.g. cimetidine, ranitidine, famotidine, nizatidine • c. Proton-pump inhibitors: reduce gastric secretions, promote healing of esophageal erosion and relieve symptoms, e.g. omeprazole (prilosec); lansoprazole • d. Promotility agent: enhances esophageal clearance and gastric emptying
Gastroesophageal Reflux Disease (GERD) Dietary and Lifestyle Management • a. Elimination of acid foods (tomatoes, spicy, citrus foods, coffee) • b. Avoiding food which relax esophageal sphincter or delay gastric emptying (fatty foods, chocolate, alcohol) • c. Maintain ideal body weight • d. Eat small meals and stay upright 2 hours post eating; no eating 3 hours prior to going to bed • e. Elevate head of bed on 6 – 8 blocks to decrease reflux • f. No smoking • g. Avoiding bending and wear loose fitting clothing
Gastroesophageal Reflux Disease (GERD) 9. Surgery indicated for persons not improved by diet and life style changes • a. Laparoscopic procedures to tighten lower esophageal sphincter • b. Open surgical procedure: fundoplication 10. Nursing Care • a. Pain usually controlled by treatment • b. Assist client to institute home plan
Hiatal Hernia 1. Definition • Part of stomach protrudes through the esophageal hiatus of the diaphragm into thoracic cavity • Types • Sliding hiatal herni • Paraesophageal hiatal hernia: ( hernia can become strangulated; client may develop gastritis with bleeding)
Hiatal Hernia • Manifestations: Similar to GERD • Diagnostic Tests • a. Barium swallow • b. Upper endoscopy • Treatment • Similar to GERD: diet and lifestyle changes, medications • If medical treatment is not effective or hernia becomes incarcerated, then surgery; usually • Fundoplication by thoracic or abdominal approach
Diverticulum • It is an outpouching of mucosa& submucosa that protrudes through a weak portion of the musculature • Clinical Manifestations • Difficulty of swallowing & neck fullness • Belching • Regurgitation of undigested food • Gargling noise after eating • Halitosis & sour taste in the mouth • May dysphagia & chest pain
Diverticulum • Management • Diverticulectomy &myoectomy for muscle • NPO until x-ray show no leakage at surgical site • During O.P. avoid trauma to carotid artery and jugular vein
Perforation • May result from stab or bullet wounds of the neck & the chest as well as from accidental puncture by surgical instrument • Clinical Manifestations • Persistent pain followed by dysphagia • Infection ,fever ,& leukocytosis • May sign of Pnuemothorax
Perforation • Management • Broad spectrum antibiotics • Nasogastric tube & suctioning • NPO – total parenteral nutrition “gastrostomy” • Closed the wound &post op management
Gastritis 1. Definition: Inflammation of stomach lining from irritation of gastric mucosa (normally protected from gastric acid and enzymes by mucosal barrier) 2. Types • a. Acute Gastritis 1.Disruption of mucosal barrier allowing hydrochloric acid and pepsin to have contact with gastric tissue: leads to irritation, inflammation, superficial erosions 2.Gastric mucosa rapidly regenerates; self-limiting disorder
Gastritis Causes of acute gastritis • a. Irritants include aspirin and other NSAIDS, corticosteroids, alcohol, caffeine • b.Ingestion of corrosive substances: alkali or acid • c.food contamination (microorganisms) Manifestations • headache, mild epigastric discomfort, • abdominal pain, nausea anorexia, vomiting • Belching, heart burn , &sour taste in mouth • If perforation occurs, signs of peritonitis
Gastritis Treatment • As a rule the patient recover in a day • NPO status to rest GI tract for 6 – 12 hours, reintroduce clear liquids gradually and progress; intravenous fluid and electrolytes if indicated • b. antacids If gastritis from corrosive substance: immediate dilution and removal of substance by gastric lavage (washing out stomach contents via nasogastric tube), • If extreme condition Gastrojejunostomy or gastric resection
Gastritis • Nursing Management • Reducing anxiety • Promoting optimal nutrition • Promoting fluid balance • Relieving pain • Chronic Gastritis • Progressive disorder beginning with superficial inflammation and leads to atrophy of gastric tissues (prolong Gastritis)
Peptic Ulcer Disease (PUD) Definition and Risk factors • Break in mucous lining of GI tract comes into contact with gastric juice , referred to as gastric ,duodenal , or esophageal ulcer • Duodenal ulcers: most common; affect mostly males ages 30 – 55 ulcers found near pyloris • Gastric ulcers:affect older persons(ages 55 – 70)
Peptic Ulcer Disease (PUD) 2. Pathophysiology • a. Ulcers or breaks in mucosa of GI tract occur with 1.H. pylori infection (spread by oral to oral, fecal-oral routes) damages gastric epithelial cells reducing effectiveness of gastric mucus 2.Use of NSAIDS: interrupts prostaglandin synthesis which maintains mucous barrier of gastric mucosa • b. Chronic with spontaneous remissions and exacerbations associated with trauma, infection, physical or psychological stress
Peptic Ulcer Disease (PUD) Manifestations • Pain is classic symptom: burning, aching hunger like in epigastric region possibly radiating to back; occurs when stomach is empty and relieved by food (pain: food: relief pattern) • Vomiting , nausea , constipation &diarrhea • Symptoms less clear in older adult; may have poorly localized discomfort, dysphagia, weight loss; presenting symptom may be complication: GI hemorrhage or perforation of stomach or duodenum
Peptic Ulcer Disease (PUD) • Treatment • Pharmacologic therapy • H2 receptor antagonist • Proton pump inhibitors • Cytoprotective agents • Antacid • Stress Reduction & Rest • Smoking Cessation • Dietary Modification
Peptic Ulcer Disease (PUD) • Surgical Management • Vagotomy • Truncal • Selective • Pyloroplasty • Antrectomy • Gastroduodenostomy • Gastrojejunostomy • Subtotal gastroectomy with anastomosis
Gastric Surgery • Gastric surgery : may be performed on patient with peptic ulcers who have life threatening hemorrhage , obstruction , perforation ,or whose condition dose not respond to medical treatment • Nursing Care • Reducing Anxiety • Increasing Knowledge • Resuming enteral Intake • Relieving pain &prevent complications • Teaching Dietary self Management
Intestinal and rectal disorders Constipation • Abnormal hardening of stool that makes difficult & some time painfull,decrease in stool volume , or retention of stool on rectum for prolonged period of time • Clinical Manifestations • Abdominal distention & intestinal rumbling • Pain & pressure • Anorexia fatigue & headache • Incomplete emptying & strain defecation
Intestinal and rectal disorders Constipation • Medical Management • Treatment of the underlying cause • High Fiber Diet & increase fluid intake • Maintain regular pattern of exercises • Laxatives & bulk forming Agents • Bran 6-12 tsp • Complications: -hypertension - hemorrhoid & fissure - fecal impaction & megacolon
Intestinal and rectal disorders Diarrhea • It is an increase frequency of bowel movement more than three times /day • Causes : - • Certain medications • Tube feeding formula • Certain metabolic disease • Viral & bacterial infectious disease • Ulcerative colitis .enteritis & chrons disease
Intestinal and rectal disorders Diarrhea • Clinical Manifestations • Abdominal cramps, distention, intestinal rumbling • Increase frequency & fluid content of stool • Anorexia , thirst , & dehydration • Fluid electrolytes imbalance • Complications:- -cardiac arrhythmia due to fluid & K loss -drowsiness & hypotension
Intestinal and rectal disorders Diarrhea • Medical Management • Treatment of underlying cause • Controlling symptoms & preventing complications • Antibiotics & antinflammatory agents • Antidiarrheal & antispasmoic agents • Nursing Managements • Assessment the ch.ch. & pattern of diarrhea • Bed rest & monitoring of fluid status • Serum electrolytes (K) • Perenial care
Fecal Incontinence • The involuntary passage of stool from the rectum • Clinical Manifestations • Minor soiling • Occasional Urgency & loss of control • Poor Control of flatus • Diarrhea ,or constipation may be present