Background and Objective
Task-shifting of HIV care and ART initiation: Three year evaluation of a mixed-care provider model for ART delivery.


Background and Objective
E N D
Presentation Transcript
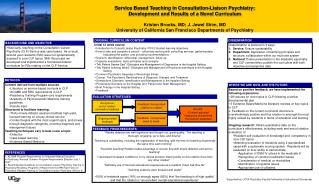
Task-shifting of HIV care and ART initiation: Three year evaluation of a mixed-care provider model for ART delivery Megan McGuire1, Jihane Ben-Farhat1, Gaelle Pedrono2, Sylvie Goossens3, Annette Heinzelmann3, Owen Chikwaza4, Elisabeth Szumilin3, Mathilde Berthelot3, Mar Pujades-Rodriguez5 1Epicentre, Nairobi, Kenya, 2 Médecins Sans Frontières , Chiradzulu, Malawi, 3 Médecins Sans Frontières , Paris, France, 4Ministry of Health, Chiradzulu, Malawi, 5Epicentre, Paris, France
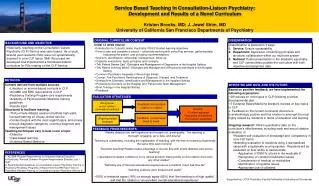
Background and Objective • Physiciancentered ART delivery models are not replicable in settings with high HIV prevalence and limited medical human resources • Utilizing mixed level cadres of staff could facilitate scaling up of care • We compared treatment outcomes of patients receiving ART and followed by different types of providers in a large HIV program in rural Malawi 2010 monthly program activity:14,000 HIV consultations, 700 program enrollments and 400 ART initiations
Methods • Eligibility criteria for nurse care: ART naïve at therapy start, in WHO stage 1 or 2, CD4 count >100 cells/μL, BMI >17 kg, on first line. • Study population: Inclusion of 10,112 adults (>15 years) who started ART between Sept 2007- March 2010. • Study definitions: ≥80% of visits by either nurse or clinical officer, <80% of visits in mixed group. • Statistical analysis: Follow-up was right-censored at the earliest of the following dates: death, transfer out, last visit or 24 months of follow-up. • Multivariable Poisson models to compare 2-year mortality and program attrition by type of provider • Sensitivity analysis: patients with BMI>18.5 kg/m2, clinical stage 1 or 2 and CD4>100
Mortality and Attrition 0.19 0.34 0.17 0.30 0.15 0.23 0.12
Association between mortality or attrition by type of provider * BMI>18.5 and WHO stage 1 or 2 and CD4>100, N=3846 CD4 count gains since ART start by type of provider, cells/μL
Discussion • Mortality was similar in the nurse and mixed care groups during the first 2 years of ART, but program retention was lower in the first group • These results support the use of a mixed care approach with well trained and supervised nurses for the provision of HIV care • Use of clear clinical criteria for inclusion and referral of patients is essential • National policies need to be adapted to ensure continuation of ART scale-up, including ART initiation and follow-up, nurse deployment for HIV care as complementary workers is essential. Limitations: Observational study based on routine monitoring data; severe or complicated patients primarily treated by or referred to CO’s. Nurses have additional responsibilities in HC. A competing risk analysis needs is to be done as a further sensitivity analysis. See poster presentation MOPE436 on six month appointments