Download
1 / 33
390 likes | 915 Views
Gross anatomy of the spinal cord. Dermatomes Dr. Katalin Gallatz. Nervous system CNS brain spinal cord PNS peripherial nerves ganglia. Spinal Cord. - b egins at foramen magnum , e nds at L 1 -L 2 intervertebral disk 58-60 cm in length. Distal e nd of the spinal cord.

E N D
Gross anatomy of the spinal cord. Dermatomes Dr. Katalin Gallatz
Nervous system CNS brain spinal cord PNS peripherial nerves ganglia
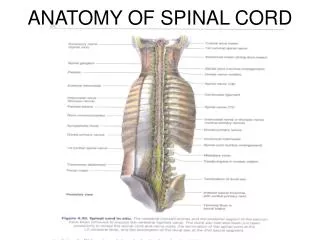
Spinal Cord - begins at foramen magnum, ends at L1-L2 intervertebral disk 58-60 cm in length
Distal end of the spinal cord • Conus medullaris: • thin, conical end of the spinal cord • the spinal cord ends at vertebral levels L1-L2 • Cauda equina (horse tail): - is the collection of lumbar and sacral spinal nerve roots that pass caudally to exit at their respective intervertebral foramen. • Filum terminale: • thin thread of fibrous tissue at end of conus medullaris • attaches to coccygeal ligament
The spinal cord is composed of the following 31 segments: 8 cervical (C) segments 12 thoracic (T) segments 5 lumbar (L) segments 5 sacral (S) segments 1 coccygeal (Co) segment - mainly vestigial
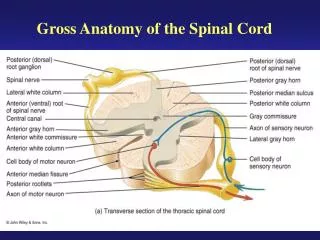
Gross Anatomy of the Spinal Cord Figure 13.3
Spinal cord • Enlargements: intumescentia cervicalis intumescentia lumbalis • 31 segments • each segment has a pair of dorsal roots and a pair of ventral roots spinal nerves
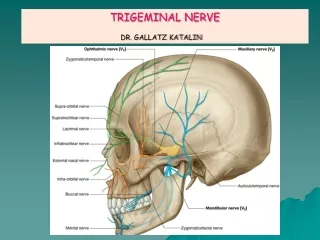
The spinal nerves consist of • - the sensory or dorsal roots, which • enter the spinal cord at each level, • - the motor or ventral roots, which emerge • from the cord at each level. • The spinal nerves are named and numbered • according to the site of their emergence • from the vertebral canal. • C1-7 nerves emerge above their respective • vertebrae. • C8 emerges between the seventh cervical • and first thoracic vertebrae. • The remaining nerves emerge below their • respective vertebrae.
- anterior median fissure is occupied by the anterior spinal artery, • - posterior median sulcus is less prominent. • anterolateral and posterolateral sulci are where the anterior and posterior nerve rootlets • emerge
Spinal meninges • Three layers • Dura mater • Arachnoid • Pia mater • Epidural space separates dura mater from walls of vertebral canal. • Subdural space separetes it from the arachnoid. • Between the arachnoid and pia mater is the subarachnoid space, filled with CSF
Meningeal Spaces Subarachnoid space-contains cerebrospinal fluid Subdural space is a virtual space Epidural space-contains fat and anterior and posterior venous plexuses
Pia mater: • - is the innermost meningeal layer, • - denticulate ligaments extend from pia mater to dura mater
Denticulate ligaments (purple) are bilateral thickenings of the collagen component of pia mater.
Cross section of the spinal cord • White mattercomposed of myelinated and unmyelinated axons • Gray mattercontain cell bodies, unmyelinated axons and neuroglia
Gray matter of spinal cord • Posterior horn contains somatic and visceral sensory neurons • Anterior hornscontain somatic motor neurons • Lateral horns contain visceral motor neurons
White Matter • Bundles of myelinated axons that run up & down • Dorsal or posterior column or funiculus • Lateral column or funiculus • Anterior columns or funiculi • Each column is filled with tracts or fascicles
The arteriesof the spinal cord comes from - anterior spinal artery - posterior spinal arteries - radicular arteries that enter along ventral roots. Anterior spinal artery supplies most of the spinal cord. Radicular arteries are branches of spinal arteries which, in turn, are branches of regional arteries (vertebral, intercostal, lumbar and lateral sacral).
The arteries of Adamkiewicz • Spinal branches (segmental radicular arteries) from the 1st and 11th intercostal arteries are large (T1 & T11) • They pass along the nerve roots to the spinal cord and reinforce the anterior and posterior spinal arteries • supply the lower thoracic and upper lumbar parts of the cord. Spinal artery at T1 (Adamkiewicz) • supplies the spinal cord only downwards Spinal artery at T11 (Adamkiewicz) • supplies the spinal cord both above and below (radicularis magna)
Spinal Veins • Spinal veins drain into theinternal venous plexus and from here the blood flows into the external venous plexus. At the end the venous blood flows into • vertebralveins in the neck, • azygos and hemiazygos veins in the thorax, • lumbar veins in the lumbar region, • lateral sacral veins in the sacral region
Dermatome is an area of skin that is supplied by a single pair of dorsal roots. Although the general pattern of dermatomes is similar in all people, the precise areas of innervation are as unique to an individual as fingerprints.
Clinical significance of the dermatomes A dermatome is an area of skin innervated by sensory neurons of a spinal nerve ganglion. Symptoms that follow a dermatome (e.g. like pain or a rash) may indicate a pathology that involves the related nerve root. The significance of a dermatome is that the nerves that travel through the particular dermatome routes affect the area in which their dermatome is located. Nerves affect the dermatome in 2 ways: sensory - felt sensation motor - ability to move
Clinically important dermatomes are as follows: C2 and C3 - Posterior head and neck C4 and T2 - Adjacent to each other in the upper thorax T4 or T5 - Nipple T10 - Umbilicus Upper extremity – C5 (anterior shoulder), C6 (thumb), C7 (index and middle fingers), C 7/8 (ring finger), C8 (little finger), T1 (inner forearm), T2 (upper inner arm), T2/3 (axilla) Lower extremity – L1 (anterior upper-inner thigh), L2 (anterior upper thigh), L3 (knee), L4 (medial malleolus), L5 (dorsum of foot), L5 (toes 1-3), S1 (toes 4, 5; lateral malleolus) S3/C1 - Anus
Spinal Taps - The needle punctures the dura and withdraws CSF - the needle is in the subarachnoid space, nearthenerves of the cauda equina, below the SC Myelography - injection of a radiopaque (opaque to x-rays) dye into the CSF - CSF appears white on a radiograph tumors, inflammation,adhesions that distort or divert CSF will be shown Fig 14.4