Download
1 / 63
670 likes | 1.59k Views
Introduction. Stillbirth rate (fetal death rate). The number of stillborn infants per 1000 infants born, including live births and stillbornsNeonatal mortality rate. The number of neonatal deaths per 1000 live birthsPerinatal mortality rate. The number of stillbirths plus neonatal deaths per 1000

E N D
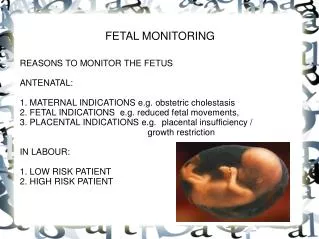
1. ELECTRONIC FETAL MONITORING By: Dr. Sahar Al-Suwailem
Consultant GYN endoscopy
KFMC, WSH
2. Introduction Stillbirth rate (fetal death rate). The number of stillborn infants per 1000 infants born, including live births and stillborns
Neonatal mortality rate. The number of neonatal deaths per 1000 live births
Perinatal mortality rate. The number of stillbirths plus neonatal deaths per 1000 total births
Infant mortality rate. The number of infant deaths per 1000 live births
3. Introduction - cont. Introduced in 1960 at Yale university with the aim of reduction in cerebral palsy
No reduction and rate is still 2-3/10000 live births (Parkes et al 2001)
FHR by NST is most common test of fetal well being
NST should not be relied upon as the sole means of establishing fetal well being (I A)
4. Cerebral Palsy Definition - a chronic neuromuscular disability characterized by aberrant control of movement or posture appearing early in life and not the result of recognized progressive disease. It may be accompanied by a seizure disorder or mental retardation or both
Causes Unknown
5. Cerebral Palsy - cont. The largest study of risk factors associated with cerebral palsy did not confirm a strong relationship between perinatal asphyxia and cerebral palsy
10% of cerebral palsy in term infants is associated with perinatal asphyxia
6. Introduction -cont. Despite widespread use
There is controversy about the efficacy of EFM
Interpretation of fetal heart rate patterns
Reproducibility of its interpretation
Management algorithms for abnormal or non reassuring patterns
7. What are the criteria's of ideal test of fetal well being? Quick
Easy to perform
Yield readily interpreted results that are reproducible
Clearly identify the compromised fetus at a stage at which intervention will improve the outcome
It should not give an abnormal result for a healthy fetus
UNFORTUNATELY this ideal test does not yet exist
8. Appropriate emergency nursing interventions Change maternal position
Give oxygen per mask @ 8-10 liters
Initiate or increase intravenous fluids (plasma expander such as ringer lactate)
Discontinue oxytocin, remove prostaglandin if possible
Vaginal examination
9. Monitoring Variables FHR- EXTERNAL MONITORING
MODES-USS (movement of fetal heart)
PHONOCARDIOGRAPHY( heart sounds)
ABDOMINAL WALL FECG (Best indirect signal source)
INTERNAL MONITORING
SIGNAL SOURCE (electrical activity of FHR)
10. Factors Affecting Test Results SLEEP CYCLES (20-40 MIN)
MEDICATIONS
EPIDURAL ANALGESIA
PARENTRAL NARCOTICS
EFFECT OF STEROIDS
(BETAMETHASONE) transiently decrease the FHR variability returned by 4-7 days and decrease in acceleration
NO EFFECT OF DEXAMETHASONE
MGSO4
11. MATERNAL SMOKING
MATERNAL HYPOGLYCEMIA
PREMATURITY - non reassuring FHR patterns may occur with up to 60 % of preterm parturient with most common abnormality being deceleration and bradycardia followed by tachycardia and flat tracing
Variable decelerations more common among preterm (55-70%) than term (20-30%) Factors Affecting Test Results - cont.
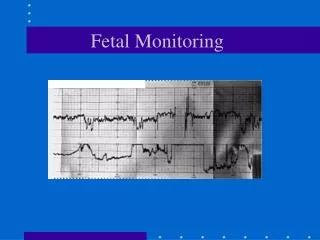
12. Uterine Activity
13. Interpretation of EFH monitoring Baseline
Baseline variability
Accelerations
Deceleration Early
Late
Variable
Prolonged
Tachycardia / Bradycardia
38. Classification of variable deceleration Reassuring
39. Atypical Features Deceleration < 70 bpm lasting > 60 seconds
Loss of variability in baseline FHR and in the trough of deceleration
Biphasic deceleration
Prolonged secondary acceleration (post deceleration smooth overshoot of > 20 bpm increase or lasting > 20 seconds
Slow return to baseline
Continuation of the baseline at a lower level than prior to the deceleration
The presence of fetal tachycardia
57. Part II - Fetal Blood Sampling Hypoxemi: Decreased oxygen content in blood
Hypoxia: Decreased level of oxygen in tissue
Acidemia: Increased concentration of hydrogen ions in the blood
Asphyxia: Hypoxia with matabolic acidosis
58. Additional tests and therapies used in combination with EFM Units employing EFM should have ready access to fetal blood sampling facilities.
Where delivery is contemplated because of an abnormal fetal heart-rate pattern, in cases of suspected fetal acidosis, fetal blood sampling should be undertaken in the absence of technical difficulties or any contraindications
60. Additional tests and therapies used in combination with EFM - cont. Contraindications to fetal blood sampling includes:
Maternal infection (e.g. HIV, hepatitis viruses and herpes simplex virus)
Fetal bleeding disorders (e.g. haemophilia)
Permaturity (<34 weeks)
Where there is clear evidence of acute fetal compromise (e.g. prolonged deceleration greater than three minutes), fetal blood sampling should not be undertaken and the baby should be delivered urgently
61. Additional tests and therapies used in combination with EFM - cont. Fetal blood sampling should be undertaken with the mother in the left-lateral position
In the presence of abnormal FHR patterns and uterine hypercintractility (not secondary to oxytocin infusion) tecolysis should be considered. A suggested regimen is subcutaneous terbutaline 0.25 mg
62. Classification of fetal blood sample results