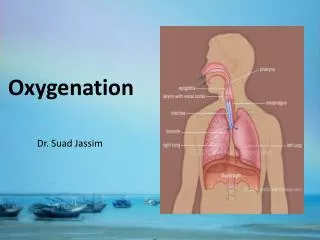
Oxygenation
Oxygenation. Chapter 40. ANATOMY AND PHYSIOLOGY REVIEW. CARDIOVASCULAR/RESPIRATORY CONNECTION BOTH SYSTEMS MUST BE FUNCTIONING FOR EITHER SYSTEM TO WORK heart structure/function lung structure/function CNS innervation to chest, diaphragm Peripheral and cardiac circulation

Oxygenation
E N D
Presentation Transcript
Oxygenation Chapter 40
ANATOMY AND PHYSIOLOGY REVIEW CARDIOVASCULAR/RESPIRATORY CONNECTION BOTH SYSTEMS MUST BE FUNCTIONING FOR EITHER SYSTEM TO WORK heart structure/function lung structure/function CNS innervation to chest, diaphragm Peripheral and cardiac circulation Adequate volume and hemoglobin Acid-base balance & regulation CO2 response/ O2 response
ALTERATIONS IN OXYGENATION PHYSIOLOGICAL → DECREASE IN OXYGEN CARRYING CAPACITY ↓ Transport HGB & HCT ↓ VOLUME R/T BLOOD LOSS ↓ Binding of O2 [CO] ↓ Intake of O2 [altitude] ↑ DEMAND [exercise, fever, illness]
ALTERATIONS IN OXYGENATION PHYSIOLOGICAL → ↓CHEST WALL MOVEMENT PREGNANCY OBESITY MUSCULOSKELETAL CHANGES [kyphosis] TRAUMA [ rib fracture] CNS ABNORMALITIES [C4 spinal trauma]
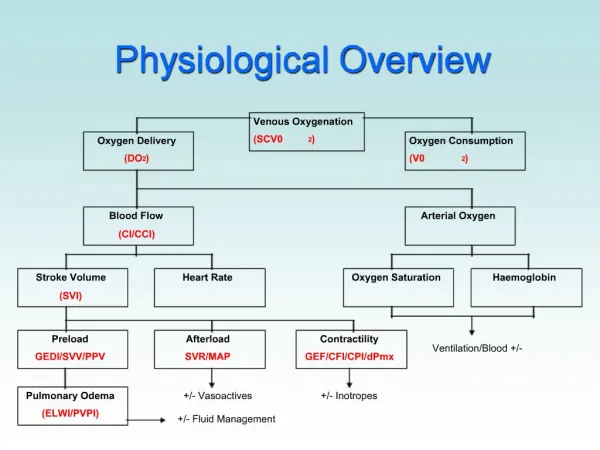
ALTERATIONS IN OXYGENATION • Physiological→ Changes in Delivery of O2 • Diffusion in lungs [alveolar] • atelectasis, ↓surface area, ↓blood supply, pressure • Secretions [pneumonia, COPD] • Transport to tissues • Cardiac output • circulation [PVD, trauma, volume, vasoconstriction] • Cardiac perfusion
ALTERATIONS IN OXYGENATION PHYSIOLOGICAL CHRONICDISEASES COPD: CO2 drive absent R/T chronic high pCO2 Dependent on paO2 drive; ↓compliance, atelectasis, ↓clearance of airways POLYCYTHEMIA: response to chronic hypoxemia CONDUCTION DISTURBANCES HEART FAILURE
ALTERATIONS IN RESPIRATORY FUNCTIONING We breathe to take in O2 and eliminate CO2 HYPERVENTILATION: in excess of what is needed to eliminate CO2 HYPOVENTILATION: inadequate to meet O2 needs OR to eliminate CO2 HYPOXIA INADEQUATE TISSUE OXYGENATION HYPOXEMIA DECREASED OXYGEN CONCENTRATION IN THE ARTERIAL BLOOD
SPECIAL OXYGEN CONSIDERATIONS ACROSS THE LIFE SPAN INFANTS AND TODDLERS SURFACTANT [newborn] Risk for URI Shorter airways OLDER ADULTS DEGENERATIVE PROCESSES Compliance, chest wall movement, accumulated pollutants, cardiac and perfusion changes, alveolar changes, cilia decrease CHRONIC DISEASE HTN, Respiratory, Cardiac, Renal…
LIFESTYLE FACTORS NUTRITION EXERCISE SMOKING SUBSTANCE ABUSE STRESS ENVIRONMENTAL FACTORS
Nursing Process • Nursing History: Ability to meet O2 needs Cardiac function Respiratory function Pain Fatigue Dyspnea Cough Wheezing Respiratory Infections Allergies Risk Factors Medications
PHYSICAL ASSESSMENT INSPECTION GENERAL APPEARANCE LOC SYSTEMIC CIRCULATION BREATHING PATTERNS CHEST WALL MOVEMENT
PHYSICAL ASSESSMENT PALPATION THORACIC EXCURSION AREAS OF TENDERNESS EXTREMITIES CAPILLARY REFILL
PHYSICAL ASSESSMENT PERCUSSION AREAS OF CONSOLIDATION AUSCULTATION NORMAL V. ABNORMAL LUNG SOUNDS
PHYSICAL ASSESSMENT DIAGNOSTIC TESTS PULSE OXIMETER PEAK EXPIRATORY FLOW RATE ARTERIAL BLOOD GASES CHEST X-RAY SPUTUM SPECIMEN PULMONARY FUNCTION TESTING BRONCHOSCOPY VENTILATION-PERFUSION LUNG SCAN [V/Q] THORACENTESIS CT / MRI
Case Study #1 • 36 yo male visiting from Austin, TX with sudden onset” dizzy, confused, headache and hard to breathe” this afternoon. No obvious trauma. No significant medical history; friend states “he’s in great shape – an athlete – he comes here to bike and climb. He’s climbing the fourteeners!” • VS: T 37.3; P90, R36, B/P 108/58, SPO2 80% on RA • Assessment: pale, anxious, confused, c/o headache. Oriented to person only. Sinus tachycardia; deep, labored resp. with fine crackles at bases. Extremities cool to touch and pale.
What’s going on? • What is abnormal? • What do you think the cause is? • What should the interventions be? • Nursing diagnosis for this patient?
Nursing Diagnoses • Activity Intolerance • Impaired Gas Exchange • Ineffective Airway Clearance • Ineffective Breathing Pattern • Risk for Infection
Goals • Pt will: • Maintain airway • Clear secretions effectively • Increase hydrations [to mobilize secretions] • Improve Oxygenation [SPO2] • Increase activity tolerance • Report decreased Dyspnea [scale 0-10] • Decrease risk factors • Show resolution/ improvement in underlying cause
INTERVENTIONS HEALTH PROMOTION VACCINATIONS HEALTHY LIFESTYLE BEHAVIOR ENVIRONMENTAL AWARENESS EDUCATION Reduce risk factors
Case study #2 • 72 yo female Denver resident c/o SOB [dyspnea], dizziness and fatigue. Family reports she seems “pleasantly confused” today. HX of DM with renal failure treated with oral Glucophage • VS: T 36.2C, P 86, R30, B/P 160/88, SPO2 90 on RA • Labs: Na+ 136, K+ 3.0, HCT 40, Hgb 14; • ABG: ph 7.32, PaO2 80, PCO2 46, HCO3- 18 • Assessment: Oriented to person, knows she is ‘not at home’. Lungs clear, respirations rapid and deep w/o use of accessory muscles. Other findings WNL for age
What to do? • Any more info you need? Labs? • What in her history raises a flag? • What is the problem? • What interventions are appropriate? • Nursing diagnoses for this patients?
Interventions • Focus on: • treating underlying cause [abx, O2] • adaptation [meds, breathing techniques] • preventing complications [TC&DB, IS] • managing Dyspnea [O2, position, activity] • Maintaining Airway [Suction, cough, IS] • Mobilizing Secretions [hydration, TC&DB, meds] • Prevent infection/complication
Case Study #3 • 18 yo DU freshman student c/o “choking”, increased thick secretions, weak productive cough. HX of CF [cystic fibrosis] • VS: T 38.2C, P100, R 36, B/P 110/70, SPO2 80% on RA • Assessment Rhonchi, rales over all lung fields, uses accessory muscles, thick yellow secretions produced with weak rattling cough. Other systems WNL
What’s going on? • Main problem? Why? • Abnormal findings? • Nursing diagnosis? • Interventions for this client? • Education/referrals?
INTERVENTIONS IN ACUTE AND CHRONIC CARE POST OPERATIVE CARE INTERVENTIONS TO PREVENT PNEUMONIA TC&DB Q2h NASAL O2 TO KEEP O2 SAT >90% IS Q2h WA SPLINT INCISION PAIN MEDICATION
Case study #4 • 28 yo female post-op trauma pt. with Rt tibia fracture, Rt rib fracture, liver laceration [repaired]. C/O “pain all over 8/10 this am. SOB [dyspnea], dizziness • VS: T 37.4C, P88, R 30, B/P [supine =118/78, sitting= 100/64, SPO2 85% on RA • Labs: Hct 58% BUN 28 mg/100 ml; others WNL • Assessment: dry mucous membranes, skin tenting, cap refill <3 sec; pulses +2 bilat and equal, RL BK cast, Rt upper abdominal incision CDI, Rt ribs bruised. Lungs CTA. Hypoactive BS X4 quadrants, rapid shallow respirations
What is wrong? • Abnormal Findings? • History? • Nursing diagnoses? • Interventions?
Oxygen • Yes, it is a medication • Can cause harm • Ordered by Physician • Standing orders - emergency
NASAL CANNULA O2 DELIVERY UP TO 6L/M (6 liters per minute) MUST BE HUMIDIFIED >4L/M ROOM AIR = 21% O2 ROOM AIR + 3L O2 = 32% O2 APPROX. 3 – 4%/LITER Potential trauma to nares, ears
OXIMEIZER • 8 – 10 LITERS PER MINUTE • DO NOT HUMIDIFY • CONTAINS A FILTER THAT HUMIDIFIES THE OXYGEN
OXIMIZER NRS 105.320 S2009
SIMPLE FACE MASK • DELIVERS OXYGEN CONCENTRATIONS AT 40 – 60% • CONTROLLED BY LITER FLOW • 5 – 8 LITERS PER MINUTE • Short term • Not for Pts with CO2 retention
SIMPLE FACE MASK NRS 105.320 S2009
NON REBREATHER MASK • DELIVERS THE HIGHEST LEVEL OF OXYGEN POSSIBLE WITH A MASK • 95 – 100% • LITER FLOW 10 – 15 LITERS PER MINUTE • ONE WAY VALVE BETWEEN RESERVOIR AND MASK • PREVENTS ROOM AIR FROM MIXING WITH O2
NONREBREATHER MASK NRS 105.320 S2009
VENTURI MASK • DELIVERS OXYGEN FROM 24 – 50% • CAN “DIAL IN” OXYGEN LEVEL • 4L/MIN = 24% • 8L/MIN = 35%
OXYGEN FACE TENT NRS 105.320 S2009