Download

1 / 24
270 likes | 1.56k Views
Noninvasive Oxygenation and Ventilation. Goals of noninvasive measures. Either short term or long term support of pulmonary function Short Term Hospital NC BiPAP for acute respiratory distress Long Term Home O2 for chronic COPDers CPAP for Obesity Hypoventilation Syndrome or OSA.

E N D
Goals of noninvasive measures • Either short term or long term support of pulmonary function • Short Term • Hospital NC • BiPAP for acute respiratory distress • Long Term • Home O2 for chronic COPDers • CPAP for Obesity Hypoventilation Syndrome or OSA
What goal for oxygen? • COPDers • Between 88 and 95% • PaO2 >= 60 • Non-COPDers • >= 92% • PaO2 > 60
O2 Saturation vs. PaO2 • 40-50-60 to 70-80-90 rule
Types of NIV • Nasal Cannula • Venti-Mask • Non-rebreathers • BiLevel • CPAP
Non-Invasive Ventilation • BiLevel • CPAP (not discussed)
Advantages to Noninvasive Ventilation • No internal traumatic complications • Decreased infections • Less interference with communication and swallowing • Less need for sedation
Indications • Well established • COPD exacerbation • Weaning in COPD patients • Acute cardiogenic pulmonary edema • Immunocompromised patients • DNI patients • Weaker indications • Asthma exacerbations • Cystic fibrosis • Hypoxemic respiratory failure • Extubation failure
NIV and COPD • RCTs have shown • 20-50% reduced intubation rate • Improved RR, dyspnea and gas exchange • Decreased length of stay • Lowered mortality • Intubated COPD patients who have failed T “piece” trials • Should be able to breath without assistance for 5 minutes • Can tolerate levels of pressure generated by NIV • Should not be “difficult” intubations
NIV and Asthma • Physiological Rationale • Decrease work of breathing • Improve exchange • Limited evidence • No consistent recommendations for trial of NIV in patients failing standard therapy
Acute Cardiogenic Pulmonary Edema • Physiology • Recruits “flooded” alveoli • Reduces preload and afterload • RCTs have shown that BiPAP/CPAP can • Improve dyspnea and oxygenation • Lowers intubation rate • Reduced intubation • Reduced LOS • Reduced mortality
Immunocompromised Patients • Mechanical ventilation in these patients have a high risk of • Nosocomial infection (VAP) and septicemia • Fatal airway hemorrhage caused by thrombocytopenia and platelet dysfunction • NIV begun in these patients before respiratory failure becomes severe may halve mortality • Greatest benefit with early initiation and single-organ failure
Post-op Patients • CPAP reduces intubation in patients after abdominal surgery (reduces atelectasis) • NIV improves outcomes in hypoxemic respiratory failure after lung resection
Predictors of NIV success in acute respiratory distress • Cooperative patient • Intact neurological function • Good synchrony with ventilator • APACHE score <29 • pH > 7.25 • Intact dentition • Air leaking well-controlled • Able to control secretions
Selection guidelines for use of NIV in acute respiratory distress • Appropriate diagnosis with potential reversibility over hours to days • Ascertain need for ventilatory assistance • Moderate to severe respiratory distress • Tachypnea (>24/min for COPD, >30/min for hypoxemia • Accessory muscle use or abdominal paradox • Blood gas abnormality • pH < 7.35, PaCO2 > 45 or PaO2/FiO2 < 200
Contraindications for NIV • Respiratory arrest/Cardiac arrest • Medically unstable (hemodynamically unstable, arrythmias, cardiogenic shock/MI, GIB, ABG pH < 7.1) • Unable to protect airway (bulbar dysfunction, AMS) • Excessive secretions • Uncooperative or agitated • Unable to fit mask (facial trauma/surgery) • Recent upper airway or GI surgery
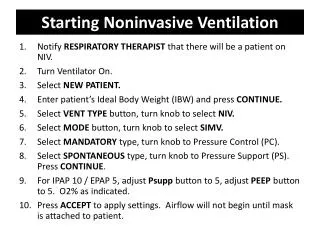
BiLevel – What is it? • IPAP (Inspiratory Positive Airway Pressure) • Excess pressure to move air into lungs • EPAP(Expiratory Positive Airway Pressure) • Increased minimum lung pressure maintained to increase alveolar recruitment • PS (Pressure Support) • PS = IPAP - EPAP
BiLevel – Setting? • IPAP • Usually 8-12 cm H2O • EPAP • Usually 4-5 cm H2O
BiLevel - Recheck • A baseline ABG should be done during initial episode of respiratory distress • Patient should be followed-up in 1-2 hours depending on condition after BiLevel NIV is placed
BiLevel – Recheck Criteria • Objective • Compare repeat ABG to baseline • PaO2/FiO2 should be > 150 after 1st hour • Gas Exchange: Oximetry, PaCO2, pH • RR, HR, BP, cough strength and ability to raise secretions should be improved • Subjective • Comfort/Discomfort • Feeling of dyspnea • Ventilatory Function • Synchrony • Tidal Volume • Airleaks • Wave form