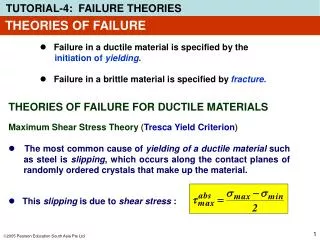
Complementary Theories: Casuistry
Complementary Theories: Casuistry. Ethics Champions August 8, 2012 Carol Bayley VP Ethics and Justice Education Dignity Health. Traditional Ethical Theories. Consequentialist theories Deontological theories Virtue theories. But wait—what’s a theory?. Systematic way of thinking

Complementary Theories: Casuistry
E N D
Presentation Transcript
Complementary Theories: Casuistry Ethics Champions August 8, 2012 Carol Bayley VP Ethics and Justice Education Dignity Health
Traditional Ethical Theories Consequentialist theories Deontological theories Virtue theories
But wait—what’s a theory? Systematic way of thinking To account for “the way things are” To answer questions (To predict or control) To determine right behavior, praiseworthiness, blameworthiness
Ethics Application of values to behavior or action
Three Ethical Theories • Consequentialist • you know if it’s good or bad by the good or bad consequences it produces • Deontologist • you know if it’s right or wrong by the characteristic of the act itself; the Categorical Imperative • Virtue • is it what a wise and prudent person would do?
What is missing from these theories A focus on cases Recognition of developmental aspects of ethical inquiry (e.g. Karen Quinlan to “futility”) Insight that some “answers” are clear, settled, agreed; others are uncomfortable, unresolved, contentious
Casuistry Evaluates action in a particular case on how closely the case resembles a “pure” or paradigmatic case Catholic manualists (casuistry is old) Depends on actual features of a case Requires clarity on paradigm cases Asks “How close is this case to the case we are sure about?”
Paradigm case: advance directive Edna Smith wrote her first Living Will in 1970, when her husband died of metastatic cancer in a hospital, where he was “fed” via an NG tube and kept alive by repeated attempts at CPR and ended up on a ventilator for 48 days. Edna wanted to be allowed to die with dignity, not as her husband had,
Paradigm case: advance directive In 1991, she read about the passage of the Patient Self-Determination Act. She procured a blank Durable Power of Attorney for Health Care, filled it out, gave it to her doctor and tore up her Living Will. The DPOA had everything important to her spelled out, and she appointed her daughter her agent.
Paradigm case: advance directive Her daughter, a nurse/doctor/lawyer, believes her mother’s wishes must be followed and promises her mother she will not die as her husband had. They revisit DPOA annually and every time one of Edna’s friends dies. In 2011, Edna has a huge mid-brain stroke; daughter asks physician to make her DNR, refuses a gastric tube and is present for ethics rounds to be sure all understand her mother’s wishes to have ventilatory support withdrawn.
Paradigm case: advance directive The physician orders withdrawal of ventilatory support under conditions most likely to prevent any suffering Edna might experience. Edna’s daughter and friends gather. Edna dies peacefully. Is what the doctor did right or wrong?
What makes this the paradigm case? Edna had capacity to make a decision Edna knew what she wanted to avoid Edna’s choice was unquestionably stable over time Edna’s agent understood her wishes and communicated them clearly Edna did not receive treatment she did not want Anything else?
What departures from this paradigm case could complicate it? Lack of capacity Lack of specificity of AD; “let me die with dignity” History of vacillating choices Unclear motivations of agent Poor communication
New case: advance directive Edna Smith read about Living Wills in 1970, when her husband died of metastatic cancer in a hospital, where he was “fed” via an NG tube and kept alive by repeated attempts at CPR and ended up on a ventilator for 48 days. Edna thought the NG tube was cruel; she agreed to withdrawal of the ventilator when several nurses confronted her.
New case: advance directive In 1991, Edna read about the passage of the Patient Self-Determination Act. She procured a blank Durable Power of Attorney for Health Care, filled it out, gave it to her doctor. She appoints both her two children as her “primary agent.” Immediately afterwards, she also made a Living Will, saying that if she were ever in a terminal condition, she wanted to be allowed to die.
New case: advance directive Her daughter, a nurse/doctor/lawyer, believes her mother’s wishes must be followed; her son lives in a distant city and figures his sister is the boss anyway. In 2006, Edna is in year five of Parkinson’s Disease with some dementia; she is capable of understanding what is happening right now, but goes along with whatever the doctor suggests.
New Case In 2011, Edna is hospitalized with her 5th bout of aspiration pneumonia. Daughter suggests hospice; son visits and is surprised by Edna’s weight loss. Son asks doctor if there is anything to be done to prevent weight loss. Doctor raises question of gastric tube to circumvent Edna’s increasing inability to swallow.
Is the doctor right or wrong to Insert a gastric tube? Choose the daughter over the son as agent? Make Edna DNR? Choose the son over the daughter as agent? Ask Edna whether she wants surgery to place a gastric tube?
Casuistry requires more than comparing case to paradigm General rules, specified by case details “listen to the patient first and to the person who knows and loves the patient next” “benefits must outweigh burdens” “do no harm”
Two Paradigm Cases Nurse gives lowest possible dose of morphine, well within the “safe” range, in order to decrease air hunger in patient with COPD. Nurse gives extremely high dose of morphine, well beyond the “safe” range, to a morphine naïve patient in order to kill the patient.
What about palliative sedation? Is it more like the first case or more like the second? What would you need to know to answer that question?
Catholic Moral Teaching--which is it? Consequences--maximize the good Deontology--certain things are always wrong Virtue--learning, habituation, wisdom Casuistry—evaluate each case
PRACTICALLY • We use all four major theories in clinical ethical cases • All four theories have virtues and flaws • Ethical theories give us a language to talk about ethics more than to do ethical reasoning. • Casuistry is our natural language but we have to be careful when we use it.