Download
1 / 18
200 likes | 352 Views
Dania Jaradat Tiffany Chang. Rabies Virus. Background Information. Family: Rhabdoviridae Enveloped (-) ssRNA virus Rod or “ bullet ” shaped Approximately 70x180 nm Coiled nucleocapsid into cylindrical structure RNA genome codes for N, P, M, G, L

E N D
Dania Jaradat Tiffany Chang Rabies Virus
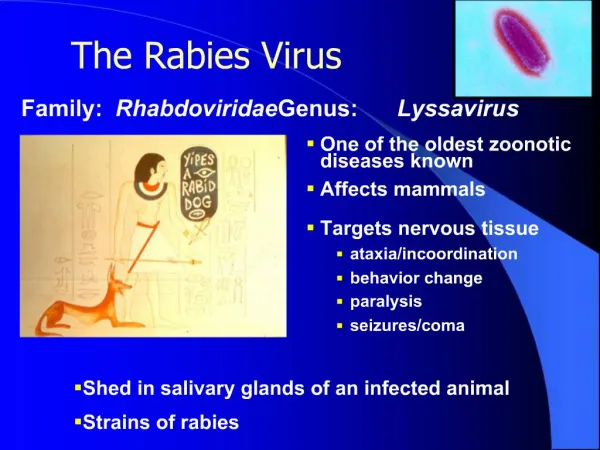
Background Information • Family: Rhabdoviridae • Enveloped (-) ssRNA virus • Rod or “bullet” shaped • Approximately 70x180 nm • Coiled nucleocapsid into cylindrical structure • RNA genome codes for N, P, M, G, L • Replication occurs in the cytoplasm inside Negri Bodies • Genus: Lyssavirus
Introduction • What is rabies virus? • An acute, central nervous system infection characterized by CNS irritation, paralysis, and death • Found worldwide, except for Antarctica due to isolation • How is it transmitted? • Animal bite – saliva of infected animals • Dogs, bats, coyotes, foxes, raccoons, skunks, etc. • Two forms: • Furious rabies (encephalitic) • Replication in the hippocampus, amygdala, anterior thalamic nuclei, and limbic cortex • Headaches, high fever, irritability, restlessness and anxiety, muscle pain, excessive salivation and vomiting • Dumb rabies (paralytic) • Replication in the neocortex • Depression, isolation, paralysis
Clinical Manifestations • Five general stages: • (1) incubation period • (2) prodrome • (3) acute neurologic period • (4) coma • (5) death (or rarely, recovery) http://www.ncbi.nlm.nih.gov/books/NBK8618/
Clinical symptoms: prodrome • Fever • Headache • Fatigue • Loss of appetite • Nausea/ vomiting • Sore throat • Nonproductive cough • Irritability • Malaise • Pain/ paresthesia (abnormal burning sensation)
Clinical symptoms: acute neurological period • Anxiety • Irritability • Confusion • Hallucination • Hydrophobia • Aerophobia • Hyperactivity • Seizures • Focal and generalized convulsions • Paralysis • Hyperventilation • Hypersalivation
Case study An 11-year-old boy was brought to a hospital in California after falling; his bruises were treated and he was released. The following day he refused to drink water with his medicine, and he became more anxious. That night he began to act up and hallucinate. He also was salivating and had difficulty breathing. Two days later, he had a fever of 40.8°C (105.4ºF) and experienced two episodes of cardiac arrest. Although rabies was suspected, no remarkable data were obtained from a computed tomographic image of the brain or cerebrospinal fluid analysis. A skin biopsy from the nape of the neck was negative for viral antigen on day 3 but was positive for rabies on day 7. The patient’s condition continued to deteriorate, and he died 11 days later. When the parents were questioned, it was learned that 6 months earlier, the boy had been bitten on the finger by a dog while on a trip to India.
1. What clinical features of this case suggested rabies? An 11-year-old boy was brought to a hospital in California after falling; his bruises were treated and he was released. The following day he refused to drink water with his medicine, and he became more anxious. That night he began to act up and hallucinate. He also was salivating and had difficulty breathing. Two days later, he had a fever of 40.8°C (105.4ºF) and experienced two episodes of cardiac arrest. Although rabies was suspected, no remarkable data were obtained from a computed tomographic image of the brain or cerebrospinal fluid analysis. A skin biopsy from the nape of the neck was negative for viral antigen on day 3 but was positive for rabies on day 7. The patient’s condition continued to deteriorate, and he died 11 days later. When the parents were questioned, it was learned that 6 months earlier, the boy had been bitten on the finger by a dogwhile on a trip to India.
2. Why does rabies have such a long incubation period? An 11-year-old boy was brought to a hospital in California after falling; his bruises were treated and he was released. The following day he refused to drink water with his medicine, and he became more anxious. That night he began to act up and hallucinate. He also was salivating and had difficulty breathing. Two days later, he had a fever of 40.8°C (105.4ºF) and experienced two episodes of cardiac arrest. Although rabies was suspected, no remarkable data were obtained from a computed tomographic image of the brain or cerebrospinal fluid analysis. A skin biopsy from the nape of the neck was negative for viral antigen on day 3 but was positive for rabies on day 7. The patient’s condition continued to deteriorate, and he died 11 days later. When the parents were questioned, it was learned that 6 months earlier, the boy had been bitten on the finger by a dog while on a trip to India.
Transmission and Mechanism of Infection • Inoculation of virus at site of wound • Replication occurs in muscle tissue near the bite • Entry into sensory nerve endings of PNS • Advances to CNS, reaching dorsal root ganglia and spinal cord • Causes trademark encephalitis • Spreads to salivary glands and other organs
Incubation period • Most commonly, lasts 3-8 weeks • But, can be as short as few days or long as >2 years • Depends on several factors • Site of bite wound • Proximity to CNS • Severity of bite • Type of virus • Quantity of virus • Age of patient • Immune status of host • The long duration of the incubation period is what makes post-exposure rabies treatment effective
3. What treatment should have been given immediately after the dog bite? What treatment should be given as soon as the diagnosis was suspected? • Post-exposure prophylaxis • Local treatment of the wound • Flushing and washing for a minimum of 15 minutes with soap, water, detergent, or iodine • Administration of Human Rabies Immunoglobulin (HRIG), if indicated • Only given once on first day of PEP regimen (designated day 0) • Dosage given calculated based on subject’s weight (20 IU/Kg body weight) • Infiltrated around the wound or intramuscularly at a different site from vaccine • Should not be given if previously vaccinated • Course of potent and effective rabies vaccine (human diploid cell, purified chick embryo cell, or rabies vaccine adsorbed) • 1 mL doses given intramuscularly in the deltoid area (adults) or in the thigh region: days 0, 3, 7, 14 • An additional 5th dose is administered on day 28 to immunosuppressed patients • If previously vaccinated, 2 doses given on: days 0, 3
3. What treatment should have been given immediately after the dog bite? What treatment should be given as soon as the diagnosis was suspected? http://www.who.int/mediacentre/factsheets/fs099/en/index.html
3. What treatment should have been given immediately after the dog bite? What treatment should be given as soon as the diagnosis was suspected? • Question the parents about patient’s history • Presence of any flu-like symptoms? (prodromal period) • Animal – wild or domesticated, location? • Once symptoms appear, very rare survival rate • Usually caused by death from respiratory failure within 7 days of the symptoms • If untreated, can lead to coma
Laboratory Diagnosis • Direct fluorescent antibody test (dFA) • Confirm the presence or absence of rabies antigen in tissue or saliva • Tests are performed on samples of: • Saliva • Serum • Spinal fluid • Hair follicles • Skin biopsy • Amplification of sample by virus isolation and reverse transcriptase polymerase chain reaction (RT-PCR) • Can confirm dFA results and detect rabies virus in saliva and skin biopsy samples
4. How do the clinical aspects of rabies differ from those of other neurological viral diseases? • Rabies differs from other neurological viruses because it has: • a complete different strategy for virus pathogenesis and spread • Rabies is spread by animal bites, thus behavioral changes (i.e. excitability, irritability, etc.) induced by the virus are important for spread • High replication of rabies in salivary glands of rabid host makes the infected animal a walking “time bomb” • 100% mortality rate (if not treated)
4. How do the clinical aspects of rabies differ from those of other neurological viral diseases? • Many common viruses that cause encephalitis have low neuroinvasiveness, but high neurovirulence • Neuroinvasive: can enter the CNS after infection of a peripheral site • Neurovirulent: can cause disease of the nervous tissue • Rabies has both highneuroinvasiveness and high neurovirulence • Neuronal spread is the definitive characteristic of pathogenesis • Examples of neurological viral diseases • Mumps virus • High neuroinvasiveness, low neurovirulence • Enters the CNS, but has mild symptoms • Herpes simplex virus • Low neuroinvasiveness, high neurovirulence • Enters the PNS (rarely CNS)
References • http://www.ncbi.nlm.nih.gov/books/NBK8618/ • http://pathmicro.med.sc.edu/virol/rabies.htm • http://www.cdc.gov/rabies/index.html • http://www.who.int/mediacentre/factsheets/fs099/en/index.html