Download
1 / 25
270 likes | 767 Views
Rabies virus family Rhabdoviridae. Jack Lam Atsuko Hil l iard Roger Salinas. What is Rabies?. Rhabdovirus family, virus Neurotropic lyssavirus. - single-stranded, neurotropic, negative-sense RNA virus .

E N D
Rabies virusfamily Rhabdoviridae Jack Lam Atsuko Hilliard Roger Salinas
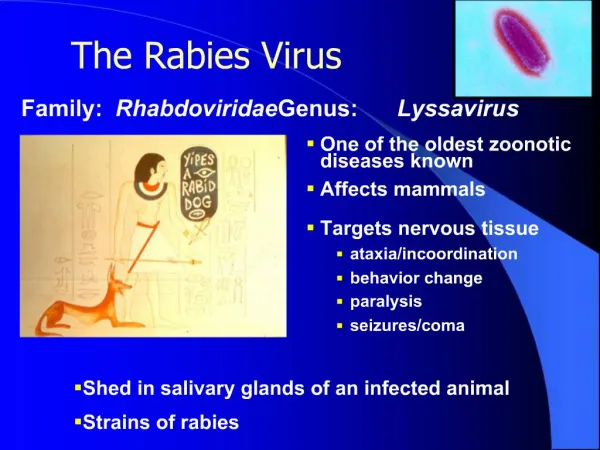
What is Rabies? • Rhabdovirus family, • virus Neurotropic lyssavirus. - single-stranded, neurotropic, negative-sense RNA virus • The mature virus has a bullet shape, a protein coat, and a lipid envelope. The outer surface of the virus is covered with thumblike glycoprotein projections
Three possible vectors • 1. The bite or scratch of an infected animal • 2. Aerosol transmission from an infected animal (usually a bat) • 3. Tissue transplants – only six recorded cases • The virus concentrates in the salivary glands, which explains why bites cause approx 99% of rabies cases worldwide
Mechanism NEUROINVASIVE • The rabies virus attacks nervous tissue and appears to replicate almost exclusively in neuronal cells • After a typical human infection by bite, the virus directly or indirectly enters the peripheral nervous system
Mechanism • The virus then travels along the nerves towards the central nervous system • During this phase, the virus cannot be easily detected within the host
Mechanism • The rabies virus replicates in CNS and then travels down nerves to the salivary glands where there is further replication
Incubation Period • The period between infection and the first flu-like symptoms is normally two to twelve weeks, but can be as long as two years • The rabies virus may lie dormant in the body for several weeks or months, but rarely much longer before symptoms appear
Incubation Period • The length of the incubation period depends on the location of the wound – a bite on the foot will have a very much longer incubation period than a bite on the face • Axonal transport of the virus to the CNS is at a rate of 3 mm per hour!
PEP – Post exposure prophylaxis • The first step is immediately washing the wound with soap and water, which is very effective at reducing the number of viral particles • The virus travel along the nerves is usually slow enough that vaccine and immunoglobulin can be administrated to protect the brain and glands from infection
Neurovirulent • This virus can cause disease of nervous tissue • Prevention of disease after exposure is only effective during the incubation period • Once symptoms have developed, death usually occurs in three to 20 days, and recovery is very rare. There are only six known cases of a person surviving untreated rabies
Case Study • An 11-year old boy was brought to the hospital in California after falling: the symptoms were treated, and he was released. The following day he refused to drink water with his medicine and he became anxious. That night he began to act up and hallucinate. He also was salivating and had difficulty breathing. Two days later, he had a fever of 40.8oC and experienced two episodes of cardiac arrest. Although rabies was suspected, no remarkable data were obtained from a computed tomographic image of the brain or cerebral spinal fluid analysis. A skin biopsy from the nape of the neck was negative for viral antigen on day 3, but positive on day 7. His condition continued to deteriorate and he died 11 days later. When the parents were questioned, it was learned that the child had been bitten on the finger by a dog 6 months earlier while on a trip to India.
Signs and Symptoms of Rabies Initial symptoms include: -a general feeling of discomfort or uneasiness - nervousness - anxiety - insomnia - depression - apathy - pain at the site of infection - fever -chills -cough -sore throat - headache - nausea -vomiting - Hydrophobia: affects 17% to 80% of rabies patients. Causes forceful, painful muscle spasms of the throat, which expel any liquids administered orally. The patient experiences apnea (interruption or halt of breathing while swallowing). Cyanosis and death can occur in this phase. Frothy saliva which drools from the patient's mouth is caused by difficulty in swallowing because of growing muscular weakness. Eventually, a variety of stimuli (the mention of water, a tactile sense or scent of water, the thought of water, etc.) can cause uncontrollable spasms and drool. Hydrophobic episodes last 1-5 minutes
Signs and Symptoms of Rabies • Rabies manifests in two forms: • Furious rabies: characterized by agitation, thrashing, biting, viciousness, choking, gagging, hyperventilation, cardiac arrhythmias, paralysis and death. • Paralytic (dumb) rabies: characterized more by paralytic symptoms, which may include apathy, apparent depression, increased blood pressure, tachycardia, confusion, hallucinations, and disorientation. These symptoms are followed by increased periods of hyperactivity, stiffness in the back of the neck, and an increase in the number of cells in the cerebrospinal fluid. Dumb or paralytic rabies ends with coma and death by respiratory failure. Most often experienced by patients who have been exposed to the virus via bats. .
Stages • Prodromal stage: Prodromal or premontive symptoms are mild and nonspecific. They include: a slight fever (100 F to 102 F), chills, malaise, headache, anorexia, nausea, sore throat (the beginnings of hydrophobia), photophobia, musculoskeletal pain, and a persistent loose cough. This stage usually lasts 2-10 days. A specific early symptom is local or radiating pain, burning, or itching, a sensation of cold, and/or tingling at the inoculation bite .
Stages • Acute neurological or excitation phase: This stage usually lasts 2 to 7 days. Patients experience nervousness, anxiety, agitation, marked restlessness, apprehension, irritability, hyperesthesia, sensitivity to loud noises, hydrophobia, excessive salivation (1 to 1.5 liters in 24 hours), lacrimation (secretion of tears), and perspiration. As the virus begins replicating in the brain, impairment of the cranial nerve occurs. This causes eye conditions: palsies, lack of parallelism of the visual axes of the eyes, asymmetrical dilation of constriction of the pupils, and an absence of corneal reflexes. At the same time, there is weakness of facial muscles and hoarseness. Systemic symptoms are severe, and they include: tachycardia or bradycardia, cyclic respirations, urinary retention, and a temperature of 103 F. The patient is often lucid between excitation and hydrophobic episodes.
Stages • Coma, or terminal phase: This phase is characterized by generalized flaccid paralysis. Eventually, the patient experiences peripheral vascular collapse, coma, and death.
Diagnosis of rabies • Rabies diagnosis can be very tricky due to the similar symptoms of other viral infections that cause encephalitis such as herpes simplex virus, mumps virus and even bacterial meningitis (syphillis). • Detection can also be difficult due to long incubation periods and is troublesome because once the onset of symptoms occur treatment is ineffective with a mortality rate of about 100% (3 rare cases of survival have been documented).
Differential Diagnosis • Rabies virus is highly neuroinvasive and neurovirulent and is almost exclusively transmitted through animal vectors through saliva exchange – here epidemiology, the vector (animal) and injury type can be a great diagnostic tool. • Rabies shows invasion into the CNS and displays rapid and severe symptoms shortly. • Herpes simplex virus are highly virulent causing severe and rapid symptoms as well but rarely enters the CNS, it usually enters the PNS. Also causes inflammation of the temporal lobe and there is no epidemiology associated with the infection. • Mumps virus high neuroinvasiveness entering the CNS but low neurovirulence displaying mild symptoms. • To distinguish viral versus bacterial infection, a spinal tap displays increases in WBC count for viruses with no detection of bacteria.
Methods of diagnosis • No single test is sufficient, a battery of test is required. • Saliva can be tested using RT-PCR • Serum and spinal fluid can be tested for antibodies for rabies virus. • Skin biopsies of hair follicles at the nape of the neck (cutaneous nerves at the base of hair follicles) can be examined for rabies antigen.
Negri Bodies (viral nucleocapsid) found in histological staining found in the cytoplasm of neurons
Methods of diagnosis – post mortem diagnosis • Direct fluorescent antibody test (dFA) – uses fluorescently-labeled anti-rabies antibody which detects rabies antigen in neural tissue viewable on a fluorescence microscope.
Treatment of Rabies Infection • Upon injury with a bite, the wound should immediately be cleansed and disinfected using normal procedures to reduce the number of viral particles entering the wound site. • A tetanus booster shot may be given to prevent secondary infection. • Antibiotics may also be given to prevent secondary infection.
Treatment Options • Following an injury due to a bite of a rabid animal, human immune globulin (HRIG) is given at the site of injury (exact weight data is used to calculate the appropriate amount) to stimulate immune cells to confer resistance and protection from the virus. • Usually vaccines are administered prior to infection but with rabies virus the vaccine is administered post infection. • This is effective due to long incubation period before the virus is able to migrate into the CNS where it replicates almost exclusively.
Treatment Options • Five 1cc (ml) follow-up injections are administered on days 3, 7, 14 and 28 following the initial day 0 injection. • These injections are selected from three possible vaccine boosters: human dipliod cell, rabies vaccine absorbed, or purified chick embryo cell culture vaccine and administered usually in the deltoid or shoulder muscle in adults (must be away from target site and readily absorbed). • If a person has already been inoculated with rabies vaccine then only 2 boosters shots are needed, one at day 0 and one at day 3. • There are no other treatment options, and the timing of treatment is crucial for protection and recovery.
References • T.H.K. Virology Notes: Rabies. http://tarakharper.com/v_rabies.htm. Accessed 11/03/07. • EmedicineHealth Online. http://www.emedicinehealth.com/rabies/article_em.htm. Accessed 11/01/07. • Department of Health Services. Rabies Fact Sheet. http://www.dhs.ca.gov/ohb/HESIS/rabies.htm. Accessed 10/31/07. • Virology Online. http://virology-online.com/viruses/Rhabdoviruses.htm. Accessed 11/01/07. • Survive Outdoors Online. http://www.surviveoutdoors.com/reference/rabies.asp. Accessed 11/01/07. • Health Scout. Health Encyclopedia – Diseases and Conditions: Rabies. http://www.healthscout.com/ency/68/738/main.html. Accessed 11/01/07. • Flint, S. J., Enquist, L. W., Krug, R. M., Racaniello, V. R., & Skalka, A. M. (2000). Principles of Virology: Molecular Biology, Pathogenesis, and Control. Washington, D.C.: ASM Press.