Awareness and Attitudes of Arab Immigrant Women Toward Breast Cancer in the UK
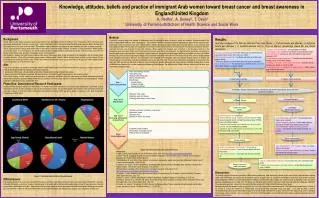
This study explores the knowledge, attitudes, beliefs, and practices of Arab immigrant women in the UK regarding breast cancer and breast awareness. Using qualitative methods, one-on-one semi-structured interviews were conducted with ten women to gain insights into their experiences and understanding of breast cancer. The research aims to identify gaps in knowledge and inform future health practices, as many Arab women face late-stage diagnoses due to lower screening rates. This study contributes to a better understanding of how cultural factors influence awareness and health behaviors among immigrant populations.

Awareness and Attitudes of Arab Immigrant Women Toward Breast Cancer in the UK
E N D
Presentation Transcript
Knowledge, attitudes, beliefs and practice of immigrant Arab women toward breast cancer and breast awareness in England/United KingdomA. Redha1, A. Dewey2, T. Dean3 University of Portsmouth/School of Health Science and Social Work • Method: • A qualitative research design was adopted; a methodology which is becoming increasing common in health care research. Qualitative research sits within an interpretative tradition to seek understanding6. The researcher selected this design to allow the participants to share with the researcher their experiences n their own words through open ended questions, reflection and probing. Data collection was conducted with one to one semi-structured audio taped interviews The interviews were conducted over a period of seven months between June-January 2009. The interview schedule for the semi-structured interviews was developed through pilot interviews (Three cases). The interviews were conducted in the language preferred by the participants, which was mainly Arabic and at a time and place that was convenient for the participants. Two approaches for recruitment were adopted to reach this particularly hidden population. A purposive sampling framework was applied with all immigrant Arab women selected from those with children attending a Saudi school from a large South of England city as well as a snowballing technique where interviewed women were asked to identify potential known participants and invite to take part, The transcriptions were analysed by the researcher (AR) using thematic analysis which is an iterative, yet systemic approach for identifying, analysing and reporting patterns (themes) within data7. This was then independently analysed by the researcher’s first supervisor (AD) who met up afterwards to discuss theme development, discuss differences and resolve issues. Following the discussion, several modifications were made which included renaming and collapsing of initial themes. The whole process of data collection, analysis and final write- up is presented in Figure One below: • Figure 2 An Overview of the Data Collection Process • Background: • Despite evidence that breast awareness leads to early detection and decreased mortality, it continues to be underused by ethnic minority women, especially Arab immigrants. There are now more than 1 million Arabs living in the UK. Research shows that Arab women are more likely to be diagnosed with breast cancer at a more advanced stage1. This advance stage of diagnosis may depend on lower frequency and rates of breast screening2, 3. Cancer screening practice among Arab women living in their native country are largely unknown, as reports of breast screening in Middle Eastern countries are sparse. To our knowledge no one yet has studied UK Arab immigrant women’s understanding of breast cancer and breast awareness with the view of informing practice and gaps in knowledge relevant to this population. • Little research is available on breast cancer incidence rates among Arab women either in their homelands or as immigrants to the UK. Breast Cancer constitutes ‘between’ 13% to 35% of all female cancer cases in Arab countries. Usually it affects younger women in Arab countries. Almost 50% are below age 50 and median age is 49-52 years4 .While in UK more than 80% of breast cancer occurs in women over 50 years old and the highest number of cases diagnosed is in the 50-64 years of age5. • Aim: • Phase One of this study is to assess the knowledge, attitudes, beliefs related to breast cancer and breast awareness practices of immigrant Arab women in the UK; this will be achieved by addressing the following objectives: • 1. Assess level of knowledge, attitudes, beliefs and practice of breast cancer among immigrant Arab women. • 2. Explore immigrant Arab women’s knowledge, attitudes, behaviours and beliefs toward breast awareness and breast screening • Phase Two is ongoing , but will utilise focus group discussions to assess the usefulness of current breast cancer and breast awareness educational material (NHS and charity produced leaflets) relevant to this population. One focus group has been conducted (different city; South England). Another is planned to take place at London in December 2011. • Phase One: Description of Research Participants: • A total of 10 Arab immigrant women were interviewed. Five women chose to be interviewed at their home, three women were interviewed in Saudi Arabia School and two women requested an interview at the researcher’s home. The sociodemographic characteristics of the interviewed women are presented in Figure1 to show the number of participants interviewed by country of birth, age group, length of residence in UK, level of education, occupation and marital status. • Figure 1: Individual characteristics of the participants • Ethical issues: • A favourable opinion for the study was obtained from the ethical committee at the School of Health Science and Social Work at Portsmouth University. Full written information, as well as a covering letter was given to all women with a stamped addressed envelope a tear off reply slip and an informed consent form in both English and Arabic. Each women received contact details to discuss the research fully with the researcher before agreeing to take part. The researcher made sure that all participants had received written information and understood the purpose and consequence of taking part. • Results: • Qualitative analysis of the findings generated four main themes: (1) Cultural beliefs and attitudes; (2) Religious beliefs and attitudes ;( 3) Systemic Barriers and (4) Personal Barriers (Knowledge toward BC and breast awareness). • Discussion: • Our findings suggest that there are a number of different factors influencing Arab women being breast aware, these include cultural attitudes, religious beliefs, lack of knowledge, personal barriers and systemic barriers. It appears there is a hunger for knowledge to know more about breast cancer and breast awareness. However, for some Arab women the inability to communicate fully in English can create a barrier to accessing health care and in particular, instigating preventive health care. This echoes the findings in earlier research that reports lower screening rates due to language difficulties8 The women also expressed a desire for a safe and comfortable environment to feel confident to discuss these issues. • Spirituality/religiosity also appears to play an important role in the lives of many of the women interviewed. This fatalist view of breast cancer is similar to the findings of a study by Thomas et al.9 among Black minority groups who associated cancer with death. Such views are likely to lead to misunderstandings about causes and treatment outcomes for breast cancer. It is also likely to deter Arab women from being breast aware or attending routine breast cancer screening. Our second phase of this study, will further explore current health promotion practice to identify potential barriers and evidence of best practice. • Cancer is a God punishment: “ It’s a punishment from Allah”. • Free mixing is a sin “ women are not allowed to be examined by male” • Don’t fight God will “that it is your fate, God determines the risk and prognosis of BC”. • Breast feeding prevent breast cancer“I am quiet sure that the breast feeding protect us from black disease”. • Believing in “Al Qada’a’ wa Al- Qadar” (act of God)“As Muslim women I believe every disease is a test from Allah,.’ • Treatment of cancer by engagement in religious activity: “Arabic women pray to avoid breast cancer ”. • Privacy & Confidentiality“I’m worried of the gossip that will be said like I have breast cancer when I don’t, this is our culture ”. ”. • Personal health not apriority“ I am feeling well while my husband and children feeling ”. • “ There is no space in our mind to think about our health as immigrants ”. • Taboo of breast cancer:“This disease has no treatment at all is , we use to call it a black disease, it’s the sign of death.”. 1. Cultural beliefs & attitudes 2. Religious beliefs & attitudes Knowledge, attitudes, beliefs and practice of immigrant Arab women toward breast cancer and breast awareness in England 4. Personal Barriers7 3. Systemic Barriers Health care system barriers Knowledge/ beliefs-related reasons Referral system is too “complicated” Need for effective cultural competent health provide:“The health care professionals should consider the growing needs of British Arab in the United Kingdom.” Insufficient understanding of the customs and culture by health authority: “no one understand us culturally” Unfamiliarity with the health system as an immigrant woman:” No idea about health care system”. Lack of knowledge regarding BC “Myknowledge about breast cancer is limited”. causes and sign & symptoms“ I think wearing bras for long time is the main cause & pain is the main sign”. Lack of knowledge regarding screening services provision. “its a bad luck to have breast screening, it’s harmful ”. Service related reasons Services barriers • Lack of female doctor in GP’s surgery: “There is no female doctor in the surgery”. • There is no privacy where the service is provided. "we don't feel that we have enough privacy”. • Health car professional communication:” No one like us ”. • Un available information: “I never found any leaflets talk about BC in Arabic ”. • Lack of female doctors“ I don’t want male doctors to examine me. • References: • 1.Aljalili, I. (2004). Arab Population in the UK. Retrieved July19, 2009, from www.naba.org.uk/content/theassociation. • 2.Sassi F, Luft HS, Guadagnoli E( 2006). Reducing racial/ethnic disparities in female breast cancer: screening rates and stage at diagnosis. Am J Public Health, 96(12):2165-2172. • 3.Smith-Bindman R, et al. (2006). Does utilization of screening mammography explain racial and ethnic differences in breast cancer? Annals of internal medicine , 144(8):541-553. • 4.Saghir, N. et al. (2007). Trends in epidemiology and management of breast cancer in developing Arab countries: A literature and registry analysis. International Journal of Surgery, 5 (4) 225-237. • 5.Breast Cancer Campaign. (2004). Breast Cancer Campaign's research achievements from: http://www.breastcancercampaign.org/whatwedo/achievements/ • 6.Creswell, J. (1998). Qualitative Inquiry and Research Design; Choosing Among Five Traditions. London, New Delhi, Thousand Oaks, Sage Publications, page 372. • 7.Braun, V., Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3 (1) 77-101. • 8.Ahmed, F., McNally, M. J. & Stewart, D.E. (2002). Breast and cervical cancer screening in Hispanic women: A literature review using the Health belief model. Women Health, 12(3), 1222-128. • 9.Thomas, V.J, Saleem, T. & Abraham, R. (2005). Barriers to effective uptake of cancer screening among black and minority ethnic groups. International Journal of Palliative Nursing, 11 (11), 562-571. • Lack of or limited English proficiency "a lot of women they can’t understand simple words”. • Isolation, poor communication with health services. “we feel that we are ignored group in Britain”. Personal barriers to health care system