Spinal Motion Restriction
Spinal Motion Restriction. Presence Regional EMS System July 2014 C.E. Objectives. Review spinal anatomy and physiology List the mechanisms of injury that cause a high index of suspicion for the possibility of spine injury. Outline the steps of patient assessment of spine injury.

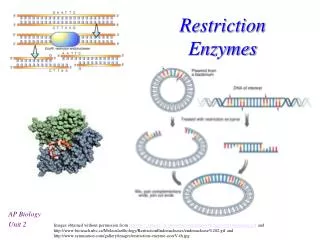
Spinal Motion Restriction
E N D
Presentation Transcript
Spinal Motion Restriction Presence Regional EMS System July 2014 C.E.
Objectives • Review spinal anatomy and physiology • List the mechanisms of injury that cause a high index of suspicion for the possibility of spine injury. • Outline the steps of patient assessment of spine injury
Objectives • Discuss the decision making process regarding Spinal Motion Restriction (SMR) •Mechanisms of injury indicating need for SMR •Emergency Rescue and Rapid Extrication •History and assessment indicating no need for SMR •Special situations indicating need for alteration of SMR • Demonstrate the process of application of SMR • Describe potential complications of Spinal Motion Restriction
Anatomy of the Human Spine • The human spine consists of 33 vertebrae • Are divided up into separate regions • Cervical region consists of 7 vertebrae • Thoracic region consists of 12 vertebrae • Lumber region consists of 5 vertebrae • Sacral region consists of 5 fused vertebrae • Coccygeal region consists of 4 fused vertebrae • Can be identified by region and location; i.e. T1 being the top vertebrae in the Thoracic region and C3 being the third vertebrae from the top of the Cervical region
Anatomy of the Human Spine • Cervical, Thoracic, and Lumber vertebrae are separated by intervertebral discs allowing for movement independent of other vertebrae • Sacral and Coccygeal vertebrae are fused and have no range of movement independent of the other bones of the structure
Cervical Spine • Consists of 7 vertebrae separated by intervertebral discs • Known as C1 (Superior Cervical Vertebrae) to C7 (Inferior Cervical Vertebrae) • Top Cervical vertebrae (C1) is known as the Atlas • This is the vertebrae connecting the head to the spine • Second vertebrae (C2) is known as the Axis • Supports the Atlas and allows the Atlas to pivot • Cervical region allows for movement of the head and neck
Thoracic Spine • Consists of 12 vertebrae separated by intervertebral discs • Known as T1 (Superior Thoracic Vertebrae) to T12 (Inferior Thoracic Vertebrae • Have facets on either side of the vertebrae that allow for interaction with the ribs • Increase in size gradually from T1 to T12
Lumbar Spine • Consists of 5 vertebrae separated by intervertebral discs • Known as L1 (Superior Lumbar Vertebrae) to L5 (Inferior Lumbar Vertebrae) • Largest vertebrae of the spinal column • Support the weight of the body and allow for movement
Sacral and Coccygeal Spine • Consists of 5 fused vertebrae (Sacral) and 4 fused vertebrae (Coccygeal) • Sacral region starts are 5 unfused bones that have fused into the Sacrum by the mid-30s • Sacral region is the base of the spine and allows for articulation with the pelvis • Coccygeal region (Coccyx) is below the Sacral region; serves a function as an attachment for various tendons, ligaments, and muscles • Coccygeal region also allows for support for sitting
Functions of the Spinal Column • Supports structure for the human body • Spinal canal of vertebrae is hollow and houses the primary route of the nervous system to the body, commonly referred to as the spinal cord • Provide structure for attachment of muscles, tendons, and ligament needed for movement
Types of Injury to the Spinal Column • Hyperextension – excessive posterior movement of the head or neck • Hyperflexion – excessive anterior movement of the head or neck • Compression – weight of head or pelvis driven into stationary neck or torso • Rotation – excessive rotation of the torso or head and neck, moving one side of the spinal column against the next • Lateral stress – direct lateral force on spinal column, typically shearing one level of cord from another • Distraction – excessive stretching of column and cord
Mechanism of Injury • The force that causes injury to the spinal column or cord • Must be a factor in patient assessment of possible spinal column injuries • Common mechanisms are automobile accidents, falls, and other blunt force traumas • Err on side of patient; if mechanism is unknown assume that there was enough force to cause an injury to the spinal column
Examples of Mechanism of Injury • A fall where a patient lands on their feet is likely to cause a compression injury • Automobile accidents with frontal collision is likely to cause both hyperextension and hyper-flexion due to the forces exerted onto the neck and spine • A hanging is likely to cause a Distraction injury due to vertebrae being pulled apart by gravity
Law of Conservation of Energy • States that energy cannot be destroyed, but can only be transferred or transformed • Applies to all mechanisms of injury • Spinal column is prone to injury due to it’s role as a supporting structure for the rest of the body • Energy from mechanism of injury can be transferred to spinal column, producing spinal injury
Assessment of Spinal Column • Consider Mechanism of Injury • If unknown and patient is unresponsive use SMR to protect Patients spinal column • Assess for DCAPP-BLS-TIC of spinal column • Look for Deformities, Contusions, Abrasions, Punctures, Penetration, Burns, Lacerations, Swelling, Tenderness, Instability, and Crepitus. • Assess PMS of patients extremities • Assess for Pulse, Movement, and Sensation of all extremities to rule out neurological or cardiovascular damage
Assessment of Spinal Column • Maintain manual control of C-spine during assessment of patient • Assessment of patient’s neck should take place prior to placement of a cervical collar • Assessment of patient’s spinal column/back should take place during log roll to backboard or prior to placement into a short backboard (KED) • Reassess PMS following placement into full Spinal-Motion-Restriction • Priapism (male erection) is an indication of spinal cord injury
Terms to remember • SMR: Spinal Motion Restrict – use of a cervical collar and backboard device to provide cervical-spine stabilization • PMS: Pulse, Movement, Sensation – assessed on extremities to check and recheck neurological and cardiovascular condition of patient • C-Spine: Cervical Spine • C-Collar: Cervical Collar
Consider SMR based on Mechanism • Suspect Spinal Column Injury with any of the following mechanisms of injury: • Motor Vehicle Crashes • Pedestrian vs vehicle • Falls • Blunt Force Trauma • Penetrating Trauma to the head, neck, or torse • Motorcycle Crashes • Hangings • Diving Accidents • Recreational accidents; i.e. ATV, waterskiing, snowboarding
Emergency Rescue • The method of extrication from a scene or vehicle when there is an immediate life threat to the patient and/or the EMS Provider • Attempt to move patient and providers out of harms way as quickly as possible • Does not provide much, if any, control of cervical-spine • Used if cases of fire, hazardous materials, or other potentially deadly threats
Emergency Rescue • To perform with one provider, ensure that patients legs will not become entangled • Place arms under patient’s armpits and use hands to grab the wrist of the patient’s opposite arm • Pull patient free of hazard; if available use second rescuer to grab patient’s legs • Attempt to regain control of cervical-spine once patient/EMS providers are safe
Rapid Extrication • Used to loosely control cervical-spine movement and move patient from a seated position in a vehicle to a backboard rapidly • Used for the following situations: • The vehicle or scene is unsafe • The patient cannot properly be assessed before removal from the vehicle • The patient requires immediately interventions • The patients condition requires immediate transport • The patient position blocks assess to another critical patient
Rapid Extrication • The first rescuer still provides manual cervical-spine stabilization, often from the back or side of the patient • The second rescuer serves as the team leader, applies the cervical collar, and moves the patients body onto the backboard • Third rescuer moves the patients lower extremities during rotation • Other rescuers can assist in movement and support
Rapid Extrication • Begin by obtaining manual cervical-spine stabilization • Place cervical collar onto patient • Use minimum three rescuers to rotate patient 90 degrees using short movements and keeping patients spine straight • Place backboard between the patient’s buttocks and seat once rotated • Move patient as a unit back onto backboard and into proper position; coordinate to maintain cervical-spine control
Special Situations • Not all patients will be able to tolerate Spinal Motion Restriction • Infants, Pediatric, Bariatric, and Geriatric patients may require alternative methods of SMR • Use padding and equipment available to maintain neutral alignment of cervical-spine • Spinal Motion Restriction may not be possible with patients who have impaled objects
Special Situations • Patients with helmets require special consideration • Athletic Helmets should be removed when: • Face mask cannot be removed in a timely fashion • Airway cannot be controlled • It does not hold the head securely • It prevents stabilization • Shoulder pads should be removed: • With helmet removal • When it does not support neutral alignment • When it impedes securing the patient to a backboard • When access to the chest is required
Special Situations • Motorcycle helmets should be removed when: • The helmet is poorly fitted to patient and allows for movement of head inside the helmet • When it causes flexion of the neck • The patients airway needs to be monitored
ALS Spinal Clearance Protocol • Region 6 Allows Advanced Providers to perform spinal clearance in order to deem a patient exempt from requiring SMR • Patient must meet criteria: • Must be over 12 years of age but less than 75 years of age • Must not have chronic neck pain • Must have Glascow Coma Scale of 15 • Cannot be complaining of neck or back pain • Must not complain of tenderness upon palpation of spine • Cannot have a distracting injury; i.e. injured extremity or burns • Must be free of drugs or alcohol • Must be able to move freely without pain or neurological compromise
Application of SMR • Application of SMR should be based on the circumstances of the call: patients will be immobilized differently based upon how they are found. • Log roll technique should be used for patient found laying supine or prone • Patients found seated should first be immobilized to a short backboard in order to maintain control of cervical-spine • Standing patients should be stood against a backboard with a rescuer holding manual c-spine, then lowered to a supine position
Log Roll Technique • First rescuer takes manual inline stabilization at the head; this rescuer directs movement of colleagues • Second rescuer applies c-collar after checking the back of the neck while a third rescuer places a backboard beside the patient • Keeping the cervical-spine inline, the patient is rolled onto an uninjured side, their back is palpated to assess for spinal column injuries, and the backboard is brought into place in the position the patient was formerly in
Log Roll Technique • Keeping the Cervical-Spine inline, the patient is rotated back onto their back, this time in position on a backboard • They are secured to the backboard first by the torso then legs; the head is secured last • Patient pulses, movement, and sensations are reassessed
SMR for the Seated Patient • The first rescuer will gain access to patient and take manual cervical stabilization • A second rescuer will apply a cervical collar after assessment of the neck • Next a short spine board will be placed between the patient’s back and the seat; palpate the spine for injuries at this time • Secure the patient to a short spine board; first use the torso straps, then the leg stirrups, and finally pad behind and secure the head
SMR for the Seated Patient • Moving the patient as a unit, rotate and move the patient onto a long backboard • Secure patient to backboard as you would normally do • DO NOT attempt to remove the short backboard from the patient
SMR for the Standing Patient • First rescuer comes behind the patient and obtains manual inline stabilization • Second rescuer applies C-Collar following assessment of neck • Third rescuer places patient against board following palpation of patient’s spine • The second and third rescuer place their arms under the armpits of the patient and grab onto the backboard
SMR for the Standing Patient • Moving as a unit, the patient is lowered to the supine position • Patient should now be secured to the backboard following standard procedures • Reassess PMS
Potential Complications of SMR • SMR may cause airway compromise due to the head and neck being in a fixed position • SMR can cause head and back pain due to position on the hard spine board • Obese patients and patients with certain illnesses may not tolerate backboards: Assess for hypoxia • Application of SMR may increase amount of time on scene; ensure that SMR will benefit your patient • Poor application of SMR may be detrimental to patient; reassess PMS prior to and following SMR
Review • If doing this CE individually, please e-mail your answers to: Shelley.Peelman@presencehealth.org • Use “July 2014 CE” in subject box. • IDPH site code: 06-7100-E-1214 • You will receive an e-mail confirmation. Print this confirmation for your records and document in your PREMSS CE record book. • Determine the Mechanism of Injury and decide whether or not SMR is needed
Answers • 25 y/o male should have full spinal motion restriction due to unknown MOI • 55 y/o driver should have full spinal motion restriction based on damage to care and chief complaint • 35 y/o does not require SMR due to no MOI • 43 y/o hanging victim requires full SMR • Driver requires Emergency Rescue then SMR when in a safe area