Bronchogenic Carcinoma: Causes, Symptoms, and Subtypes
370 likes | 778 Views
Learn about bronchogenic carcinoma, the most common lung cancer originating from bronchial cells. Explore its etiology, classifications, and clinical manifestations.

Bronchogenic Carcinoma: Causes, Symptoms, and Subtypes
E N D
Presentation Transcript
BronchogenicCarcinoma By Dr. Khaled M. Abdel Aal Ass. Prof. of Cardiothoracic surgery Sohag University
Brochogenic carcinoma • The most common carcinoma of the lung • originate in (from) normal epithelial cells of bronchus. • So we also call it : carcinoma of the bronchus (bronchial carcinoma).
Brochogenic carcinoma • Other 1ry lung tumors are: • carcinoid tumors. • mucous and salivary gland tumors: adenois cystic carcinoma, mucoepidermoid carcinoma, and mixed salivary gland tumors. • sarcomas.
Brochogenic carcinoma • Brochogenic carcinoma is also called Lung cancer. • It is a frequent and important neoplasm in both developed country and developing country.
Brochogenic carcinoma • It now stands as one of the commoner cause of death from cancer. • in fact, it is the most common cause of death in all men with cancer.
Etiology and pathogenesis • Cigarette smoking • Occupational associations: asbestos, uranium( in miners), arsenical fumes, nickel,radon gas ects. • Other factors include air pollutions , ionizing radiation . • Nowadays It is reported that tuberculosis is associated with the incidence of lung cancer.
Etiology and pathogenesis • The nature of interaction of these environmental factors and the cells of the respiratory tract, as well as the subsequent development of carcinoma is not fully understood. • Perhaps It is related to: damage to cellular DNA; alteration in cellular oncogene expression; tumor-derived factors that stimulate cellular division.
Etiology and pathogenesis • Chronic inflammation of the lung, such as from interstitial fibrosis and areas of scarring is associated with the occurrence of adenocarcinoma. • Genetic factors also involve the formation of lung cancer.
Gross characteristics • Bronchial carcinoma occurs more frequently in the right lung than in the left. in a ratio of approximately 6:4 • the upper lobes are involved more often than the lower lobes and • the middle lobe is involved the least frequently of all in the upper lobes. • there is a predilection for the tumor to be located in the anterior segment
Classifications • According to anatomy: • According to histologic classification:
Classifications • According to anatomy: (1)Central lung cancer: mostly is squamous cell carcinoma and small cell carcinoma. (2) peripheral lung cancer: mostly is adenocarcinoma.
Classifications • According to histologic classification: 1. Small cell lung cancer(SCLC) and 2. Non-small cell lung cancer(NSCLC). NSCLC includes: Squamous cell carcinoma, large cell carcinoma adenocarcinoma adenosquamous carcinoma.
Squamous cell carcinoma: • It is the most common subtype. • It arises from altered bronchial epithelium. • It is related to cigarette smoking. • Cavitation can occurs. • Adenocarcinoma: • It arises from the submucosal glands, • located in peripheral airways and alveoli. • Peripheral adenocarcinomas are usually well-circumscribed, grey-white masses that rarely cavitate.
Large-cell carcinoma: • are usually located peripherally. • They can be quite large and not infrequently cavitate. • They have large nuclei,prominent nucleoli,abundant cytoplsma. • There are two types , Giant-cell carcinoma and clear-cell carcinoma. • Adenosquamous: • There are definite features of adenocarcinoma and squamous ce carcinoma.
Small cell carcinoma: • has three subtypes , oat-cell carcinoma, intermediate cell type and combined oat- cell carcinoma. • SCLC belongs in a group of tumors derived from neuroendocrine cells that are responsible for the production and secretion of specific peptide product. • they may related to paraneoplastic syndrome.
Brochogenic carcinoma • Clinical manifestationThe manifestations in patients with carcinoma of the lung are dependent upon those as follow
Clinical manifestation • 1) the anatomic location of the primary tumor • 2) the compression and extension of the tumor to the surrounding structures • 3) the presence of metastasis • 4) systemic effects due to hormonal syndromes produced by the neoplasm
Clinical manifestation A. Local (bronchopulmonary) manifestations: • early symptoms arising from: • involvement of the lung are due to irritation. • ulceration or obstruction or a combination of these a bronchus and • septic complication with in the lung parenchyma
Local (bronchopulmonary) manifestations: 1). irritative cough . 2). hemoptysis: generally episodic blood_streaking of the sputum, was present in 57% of the patients and way be massive 3). chest pain.
4) other symptoms: • chest distress • wheeze • stridor • short breath • fever, • dyspnea resulted from the obstruction of main bronchi by a large tumor.
B. Advanced (extrapulmonary but intrathoracic) manifestations: • The symptoms of advanced stage occur as the result of growth of the tumor beyond the confines of the lung . • the symptoms are due to involvement of the pleura. chest wall mediastinal structures and contigueus nerves. Or to distal metastasis
B. Advanced (extrapulmonary but intrathoracic) manifestations: • 1)paralysis of the diaphragm due to involvement of the ipsilateral phrenic nerve. • 2) Hoarseness due to paralysis of a vocal cord as the result of involvement of the left recurrent laryngeal nerve or rarely of the right recurrent laryngeal nerve
B. Advanced (extrapulmonary but intrathoracic) manifestations: • 3) Superior vena caval syndrome: directly related to obstruction of venous drainage of the head neck and upper extremities with a concomitant increase in venous pressure • 4) horner syndrome
B. Advanced (extrapulmonary but intrathoracic) manifestations: 5). Sever pain in the chest wall due to direct involvement of the chest wall by tumor mass. 6). pleural effusion from metastatic involvement of the pleura and it results in severe dyspnea 7). Pericardial effusion.
B. Advanced (extrapulmonary but intrathoracic) manifestations: • Pancoast: • a special and well –recognized sit for bronchogenic carcinoma involves the apex of the lung(superior sulcus tumor of pancoast in this position. • the tumor can infiltrate the upper mediastinum and involve the cords of the bronchial plexus and cervical sympathetic. • symptoms include pain in the shoulder and arm as well as in the axilla, the inner side of the upper arm and in the scapular.
C. Extrapulmonaryextrathoracic metastatic manifestations.. • Including metastasis to other organs, such as brain, • central nervous system, • skeleton system, • liver, • adrenal glands and • lymph nodes ects
D. Extrathoracicnonmentastastic symptoms (paraneoplastic manifestations): • The majority of these manifestations are the result of the secretion of endocrine or endocrine-like substances by the tumor
Paraneoplastic syndromes include: • Hypertrophic pulmonary osteoarthropathy • hypercalcemia • Inappropriate antidiuretic hormone secretion syndrome • Polymyositis • Subacute cerebellar degeneration • Peripheral neuropathies and • Cushing’s syndrome ects.
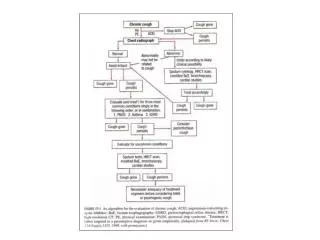
DIAGNOSIS • x-ray examination. • CT chest. • MRI chest • cytological examination of sputum. • Bronchoscopic examination. • Mediastinoscopy. • Needle biopsy. Percutaneous transthoracic • Lymph nodes biopsy. Supraclavicular,cervical, axillary. • Pleural effusion examination. • Thoracic exploration.