Download
1 / 30
380 likes | 1.34k Views
Endometrial Carcinoma. Fuat Demirkıran, MD Istanbul University, Cerrahpaşa School Of Medicine, OB&GYN Department, Gyn Oncology. In developed countries, cancer of the uterine corpus is the most common malignancy seen in the female pelvis today

E N D
Endometrial Carcinoma Fuat Demirkıran, MD Istanbul University, Cerrahpaşa School Of Medicine, OB&GYN Department, Gyn Oncology
In developed countries, cancer of the uterine corpus is the most common malignancy seen in the female pelvis today It is the fourth most common cancer in women.
Gynecologic malignancy N: 1730 CTF Gynecol Oncol 2004
EPIDEMIOLOGY and Risk Factors The median age for adenocarcinoma of the uterine corpus is 61 years, with the largest number of patients noted between the ages of 50 and 59 years. Approximately 5% of women will have adenocarcinoma before the age of 40, and 20% to 25% will be diagnosed before the menopause.
EPIDEMIOLOGY and Risk Factors The use of combination oral contraceptives (OC) decreases the risk of developing endometrial cancer. Cigarette smokingapparently decreases the risk of developing endometrial cancer. The RR decreased by about 30% when one pack of cigarettes was smoked per day
increased risk obesity increases the risk.....related to depressed SHBG in obese women nulliparity and late menopause have increased risk .....related to unoppesed estrogen · DDM and hypertansion are frequently associated with EC· The use of continuous estrogen increases the risk of EC· Tamoxifen.......related to its estrogenic effect on endometrium · PCO· Granulosa cell tumor
Risk factors for Endometrial cancer Risk factors Risk Obesity Overweight 21-50 lb 3´ >50 lb 10´ Nulliparity Compared with 1 child 2´ 5 or more children 3´ Late menopause Age >52 yr 2.4´
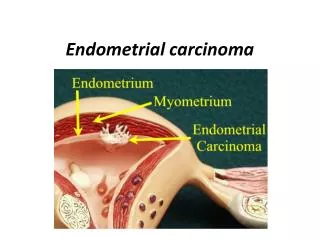
Endometrial cancer filling endometrial cavity Endometrial cancer spreading cervix
1. abnormal uterine bleeding in premenopausal period (prolonged and heavy menstruel periods and intermenstruel spoting may be related to EC.) 2. postmenopausal bleeding in postmenopausal period as the patient’s age increases after the menopause, the probability of EC with uterine bleeding increases progressively. Symptoms of Endometrial Cancer
Distribution of endometrial carcinoma by stage (surgical) Stage Patients I 73 % II 12 % III 12 % IV 3 %
Classification of Endometrial Cancer Endometrioid adenocarcinomas (Type I) Usual Secretory Villoglandular or papillary With squamous differantiation Special(non-enometrioid) variant carcinomas(Type II) Papillary serous (UPSC) Clear cell(CCC) Mucinous Pure squamous cell Mixed Undifferentiated
Diagnosis of Endometrial Cancer Cytology Endometrial cytology to make the diagnosis of EC have been less successful than sampling. only 1/3 and ½ of the patients with EC have abnormal c-v smear. Hysterograhpy and hysteroscopy are adjuvants methods in making the diagnosis of EC USG is a diagnostic tool particularly in postmenopausal women to diagnose endometrial pathology and to evaluate depth of MI of EC Tumor markers and MRI Endometrial sampling(Biopsy)
Which technique forendometrial biopsy ? D&C Pipelle-endorette Hysteroscopy
D&C the oldest technique reasonable accuracy rate need general anaesthesia complications Gold-standard technique !
False negative rates of D&C are as high as 6 and 10%. • It is found that in approximately 60% of the D&C procedures, less than half of the uterine cavity is curetted Brooks et al, Grimes et al Am Obstet Gynecol 1988, 1982 Stock et al. Am J Obstet Gynecol 1975
Pipelle-Endorette doesn’t need anaesthesia inexpensive easily used the rate of adequate sampling! histopathologic agreement with others techniques!
The Rates of Sufficient Endometrial Sample with Pipelle (-endorette) Stovall et al., 1991......Cancer............... 98% Fothergill et al., 1992......All pathology..... 84% Momerger et al., 1998......All pathology.... 95% Monganiello et al.,, 1998..... All pathology..... 99% Thanuja ve ark, 2000.....All pathology..... 89% Epstein et al., 2001....All pathology.........71 % The failure rate of endometrial sample .......1-30 % The false negative rate........5-15 %
Hysteroscopy end-point diagnostic work-up for endometrial pathology False negative rate 3%
PROGNOSTIC FACTORS IN ENDOMETRIAL ADENOCARCINOMA Histologic type (pathology) Stage of disease Histologic differentiation Myometrial invasion Peritoneal cytology Lymph node metastasis Adnexal metastasis
Stage and five-year survival in endometrial cancer Stage Survival I 86 % II 66 % III 44 % IV 16 %
Tumor differentiation and 5-year survival rate stage I (surgical) Grade Survival 1 94% 2 88% 3 79%
Relationship between depth of myometrial invasion and 5-year survival rate MI Survival rate <1/3 82.4 % 1/3-1/2 78.0 % >1/2 66.8 %
FIGO 2009 IA IB II IIIC1 IIIC2
Treatment • Total abdominal hysterectomy (TAH) + Bilateral salpingo-oophorectomy + pelvic and paraaortic • lympadenectomy should be done • After getting pathologic results , adjuvant treatment is being decided according to risk factors
Adjuvant Therapy Following Surgery IAIBICII ve> Ex-RT Br-RT ? Ex-RT Ex-RT Ex-RT Ex-RT: External radiotherapy Br-RT: Brachytherapy
Treatment Low-risk = stage Ia / Ib + grade I-II ( myometrial involvement < 1/2 peritoneal cytology negative No more therapy lymph node negative ) High- risk = Other conditions greater than low-risk papiller / clear cell Adjuvant Radiotherapy (Pelvic / paraaortic )
Treatment of Advanced Stage Endometrial Carcinoma Surgery TAH +BSO Cytoreduction Pelvic & para-aortic Lymphadenectomy Adjuvant Therapy..RT, CT & hormone
Treatment Treatment of patients with stage III-IV disease must be individualized; however, in most instances hormonal treatment or chemotherapy, or both, must be used in addition to surgery and radiation therapy.