Download

1 / 69
700 likes | 1.43k Views
Carcinoma Oesophagus. By Nishi Mary Joseph. ETIOLOGY….

E N D
Carcinoma Oesophagus By Nishi Mary Joseph
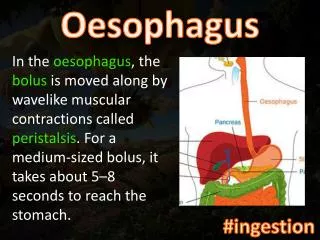
ETIOLOGY…. Alcohol Tobacco Nitrosamines Malnutrition Vitamin deficiency Anemia Poor oral hygiene C/c ingestion of hot foods and Beverages
Premalignant conditions… • Achalasia • Reflux esophagitis • Hiatal hernia • Barrett’s esophagus • Irradition esophagitis
Plummer-Vinson syndrome • Leukoplakia • Esophageal diverticula • Ectopic gastric mucosa • Familial --- keratosis palmaris et plantaris
How the patient presents?... • AGE: 6th or 7th decade COMPLAINTS : * insidious onset *non specific retrosternal discomfort *indigestion *dysphagia
Symptoms contd.. • Constant pain—somatic stuct. Invasion • Regurgitation and aspiration • Coughing related to swallowing --tracheo-esophageal fistula Hoarseness –RLN affection
# AS TUMOR ENLARGES…… *Progressive dysphagia *weight loss *odynophagia *chest pain *hemetemesis
PATHOLOGY • Squamous cell carcinoma—95% • Adenocarcinoma—2.5-8% • Rare types--
SQUAMOUS CELL CARCINOMA • 3 MORPHOLOGIC PATTERNS • Protruded-60%-- a polypoid exophytic lesion
Flat-15% *diffuse infiltrative form *spread within wall of esophagus *thickening, rigidity, narrowing of lumen
Excavated *necrotic cancerous ulceration *excavates deeply
MOST ARE MODERATE TO WELL DIFFERENTIATED 50% in middle1/3…30% in lower 1/3 20% in upper 1/3
ADENOCARCINOMA • Increasing in frequency • Distal 1/3 • Male : female = 3:1 • Origin---- 1)Barrett’s mucosa 2)esophageal submucosal glands 3)heterotropic islands of columnar epithelium
Macroscopically • Appear as FLAT or RAISED patchesof otherwise INTACT mucosa • Large nodular masses • Diffusely infiltrative • Deeply ulcerative
Microscopy:: • Mucin-producing glandular tr. Showing intestinal type feat. • Diffusely infiltrative signet-ring cells of gastric type
SQUAMOUS CELL CARCINOMA • Moderately differetiated
ADENOCARCINOMA • Intestinal type
RARE VARIETES • Adenoid cystic • Malignant melanoma • Anaplastic small cell • Carcinosarcoma
SPREAD Locoregional • Upper1/3 and middle 1/3---tracheobronchial tree ,aorta , left RLN • Lower 1/3---diaphragm, pericardium , stomach
LYMPHATICS • CERVICAL deep cervical paraesophageal posterior mediastinal tracheobronchial LOWER paraesophageal celiac splenic hilar
Distant spread • Liver • Lungs
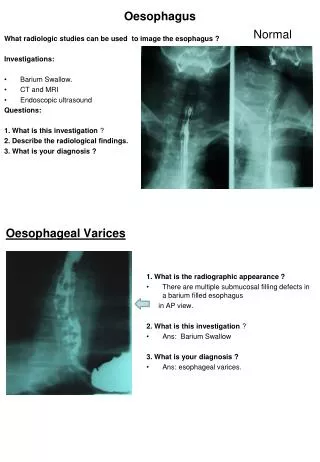
INVESTIGATIONS • Barium swallow • Chest X-ray • Esophagoscopy with biopsy and brushings • CT chest and abdomen • Bronchoscopy
Additional… • MRI • Bone and brain scan • Staging mediastinoscopy if specific symptoms or findings…..
Barium swallow • Irregular mucosal filling defect • Narrowing of lumen at site of lesion • Dilatation proximally
Upper border resembling shelf • Annular lesion—narrowed lumen irregular mucosal outline • Angulation of axis of tumor above and below tumor---spread to extraesophageal sites
CHEST X-RAYS • Air-fluid level in the obstructed esophagus in the postr. Mediastinum • Dilated esophagus • Abnormal mediastinal soft tissue—adenopathy
Pleural effusion • Pneumonitis • Lung abscess • Pulmonary metastasis • CAN BE NORMAL EVEN IN ADVANCED DISEASE
SQUAMOUS CELL CARCINOMA • Protruding • Ulcerating
CT CHEST AND UPPER ABDOMEN • Usually used for staging of the disease • Wall thickness (nl-5mm) • Direct mediastinal invasion by tumor • Regional lymphadenopathy
Metastasis –lung liver adrenal and distant nodes • ESOPHAGEAL ENDOSONOGRAPHY To determine wall penetration and mediastinal invasion—more accurate
BRONCHOSCOPY • Upper and mid esophagus • Bcoz may invade tracheobronchial tree • Positive findings *distortion of bronchial lumen *blunting of carina *intra –bronchial tumor
TNM STAGING • Done using CT • DIVIDES ESOPHAGUS INTO 4 SECTIONS • 1)CERVICAL-15-18cm.lower border of cricoid cartilage to thoracic inlet • 2)UPPER THORACIC—24cm. thoracic inlet to carina
Contd….…. • 3)MIDDLE THORACIC—32cm.carina to ½ the distance to the esophagogastric junction • 4)LOWER THORACIC—40cm.to the esophagogastric junction • REGIONAL LYMPH NODES • CERVICAL --cervical and supraclavicular nodes
THORACIC --mediastinal and perigastric LN along lesser curvature ,fundus,left gastric artery • THORACIC --mediastinal and perigastric LN along lesser curvature ,fundus,left gastric artery • THORACIC --mediastinal and perigastric LN along lesser curvature ,fundus,left gastric artery • THORACIC --mediastinal and perigastric LN along lesser curvature ,fundus,left gastric artery
PRIMARY TUMOR(T) • TX---- can not be assessed • T0 ---no evidence of primary tumor • Tis---high-grade dysplasia • T1 ---invades lamina propria (T1a) muscularis mucosa(T1a) submucosa(T1b) • Does not breach submucosa
T2 ---invades muscularis propria • T3 ---invades periesophageal tissues • T4 ---invades adjacent structures
REGIONAL LYMPH NODES (N) • Nx ---regional nodes cannot be assessed • N0 ---no regional node metastases • N1 ---regional node metastases
DISTANT METASTASIS (M) • Mx ---mets cannot be assessed • M0 ---no distant metastases • M1a ---non-regional lymph node metastases • M1b ---other distant metastases
STAGING • Stage 0---Tis N0 M0 • Stage l--- T1 N0 M0 • Stage lla--T2 N0 M0 T3 N0 M0 Stage llb—T1 N1 M0 T2 N1 M0
Stage lll –T3 N1 M0 T4 any N M0 • Stage lVa –any T any N M1 lVb –any T any N M1b
DIFFERENTIAL DIAGNOSIS • Benign strictures • Benign papillomas • Polyps • Granulomatous masses
TREATMENT • Surgery • Radiotherapy • Chemotherapy • Combination
UNRESECTABILITY • Direct spread to tracheobronchial tree or aorta • Esophageal fistula • Hoarseness of voice • Primary tumor >10 cm.
CHEMOTHERAPY • Combination chemo: • Cisplatin,bleomycin,vindesine or methotrexate