
External Ear: Anatomy, Pathology, and Infections
E N D
Presentation Transcript
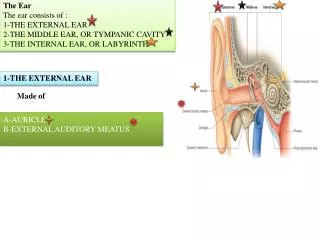
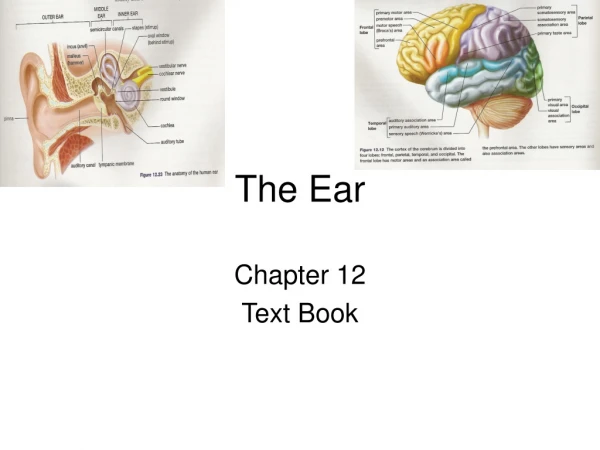
General compartments • External • Middle • Inner
External ear Embryology: • Condensation of the mesoderm of the 1st and 2nd pharyngeal/brachial arches occurs to give rise to 6 hillocks of His • 20th week gestation: It has reached adultshape • 9 years: reach adult size (this is the age of performing plastic surgery)
Anterior part: Auriculotemporal branch of mandibular branch of trigeminal (V) • Posterior and central part: auricular branch ofVagus Nerve (X), Facial nerve (VII) • Posterior and inferior part: cervical C2, C3 • Understanding innervation is important to understand referred ear pain
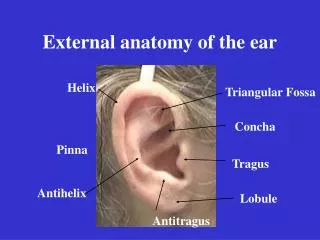
Pinna embryology • Condensation of the mesoderm of the 1st and 2nd pharyngeal/brachial arches occurs to give rise to 6 hillocks of His • 20th week: It has reached adultshape • 9 years: reach adult size (this is the age of performing plastic surgery)
Congenintal anomalies of the Pinna • Preauricular tag • Remnant of one of the hillocks. • Uncertain risk factor for hearing loss. • Preauricular sinus • results from improper fusion of the 1st & 2nd brachial arches • May be associated with branchio-oto-renal syndrome • Surgery is only indicated when it is complicated by recurrent infection or abscesses • Microtia: underdeveloped ear pinna • Bat ears: protruding ears, loss of antihelix
Infections of the auricle • Erysipelas: • infection of the overlying skin • Caused by group A beta hemolytic strep. • Rapid treatment with oral or IV antibiotic • cellulitis (infection of the soft tissue) • Cellulitis of the ear typically results from a spreading otitis externa or a penetrating injury. • It is distinguished from perichondritis by the lack of induration • Rapid treatment with Anti-staph oral or IV antibiotic • Perichondiritis to chondritis : • represent infections of the auricular perichondrium or cartilage • infection involving the cartilage itself of the auricle & external auditory canal. • The lobule, which contains no cartilage, is spared • Most common cause is Pseudomonas aeruginosa
Relapsing Polychondritis • Auto-immune disease • Pathophysiology: Chronic multisystemic Inflammation of types of cartilage and may involve other proteoglycan-rich structures, such as the eyes and the cardiovascular system. • presentation: • acute phase: fever • sudden sever painful uniform swelling and erythema of the auricle • Chondritis rapidly develops and resolves in 5-10 days • Spares: external auditory canal, lobule
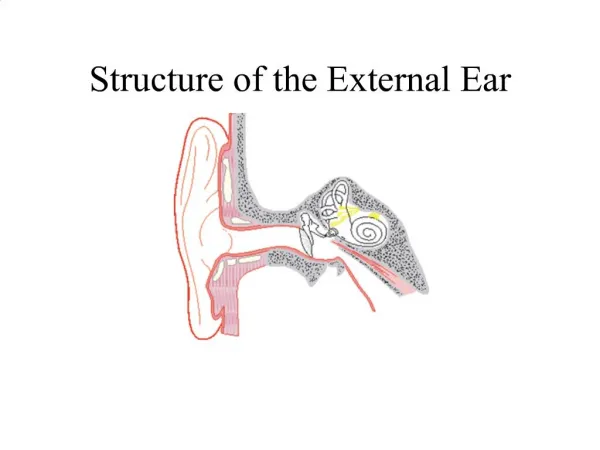
External auditory canal anatomy • It is tortuous S shaped to protects the Tympanic membrane • Dimensions: 24 mm in length from the concha to the Tympanic membrane • Bony part: 2/3 of the canal = 16 mm • Cartilaginous part:1/3 of the canal = 8 mm • Made of yellowelastic fibrocartilage • Auditory canal constrictions: • at the junction of the cartilaginous and bony portions • the isthmus • The isthmus: • The narrowest point of the EAC, 5 mm from the tympanic membrane, which is taller more than wider (important note for foreign body retrieval)
Cerumen • consists of desquamated epithelium mixed with the sebum produced from sebaceous glands and the watery secretions of modified apocrine sweat glands (apopilo-sebaceous unit) • acidic: bacteriostatic + fungostatic • contains lysozymes which are bactericidal
External auditory canal infections • Furunculosis • Furuncle is a localized abscess of the apopilo-sebaceous unit • Most common organism: S. aureus • Treatment: • Analgesia • Anti-staphylococcal oral and topical antibiotics should be administered. • A fluctuant lesion should be incised and drained under local anesthetic.
Otitis externa • Acute otitis externa affects approximately 4-8/1000 per year. • Approximately 10% of the population during their lifetime. • Approximately 80% of cases occur in the summer, particularly in warm, humid environments. • Other predisposing factors include anatomic obstructions of the ear canal (e.g., stenosis, impacted cerumen), hearing aid or ear plug use, self-induced trauma (e.g., by cotton swabs), and swimming. • Systemic: Immune compromise, DM. • Bacterial > Fungal (only 2%)
Otitis externa • Most common micro-organism: Pseudomonus aeruginosa • Second most common: Staph species (epidermidis + aureus) • Presentation: • Pain: due to high innervation, closely adherent skin • May be severe and is exacerbated by manipulation of the auricle or the tragus (due to cartilage continuity) • Discharge: scanty… • Aural fullness: due edema, discharge. • Treatment : • Frequent aural toileting • Local antibiotic • Analgesics • Avoid water contact
Fungal otitis externa (otomycosis) Aspergillus • Aspergillus accounts for 80-90 % of cases with Candida being responsible for the remaining 10-20%. • Presentation: Itchiness, Pain, aural fullness. • Treatment : • Frequent aural toileting • Local antifungal • Avoid water contact Candida
Malignant (Necrotizing) otitis externa • Malignant Otitis Externa: otitis externa + osteomyelitis of the tympanic plate of the temporal bone which may extend to involve skull base • Clinical Presentation: • Persistent Otalgia more than 1 month • Persistent Otorrhea with granulation tissue • Persistent Otorrhea in the immunocompromised patients (Diabetics with microangiopathy and cellular immune dysfunction), HIV. • Deep-seated aural pain (pain out of proportion to examination findings). • Most cases are caused by P. aeruginosa followed by S. aureus • Diagnostic: • CT scan with IV contrast • MRI • Technetium-99m bone scanning
Malignant (Necrotizing) otitis externa Treatment: • Regular aural toilet • Blood sugar control • Correct immunodeficiency if possible • Pain killer • Infectious disease consult • IV antibiotic for 6 weeks, with anti-pseudomonal coverage Prognosis: • Mortality is 5-20%
Herpes Zoster Oticus • prodrome of otalgia, which may be severe. • A vesicular eruption is seen in the canal and concha. • Ultimately, these vesicles rupture and form crusts. • Etiology: • After primary infection (chickenpox), varicella-zoster virus is harbored in a latent state in sensory ganglia, and reactivates with infection spreading along dermatomes. • Harbored in the facial nerve VII and the vestibular ganglia of VIII • A subgroup of patients manifest Ramsay Hunt syndrome: SNHL, tinnitus or vertigo or both, Palsy: lower motor neuron palsy of the ipsilateral facial nerve • 2nd commonest cause of lower facial nerve palsy after bell's palsy (9%) • Prognosis for facial nerve recovery worse than Bell’s palsy (only 60% regain normal function, where as up 90% regain normal function in bell’s palsy). • Symptoms: • Auricular pain: the 1st symptom to appear • Vesicular Rash: location: concha, EAC, mucosa of the palate, anterior 2/3 of the tongue • Treatment: • acyclovir or valacyclovir • High-dose steroids • Corneal protection