Download
1 / 39
390 likes | 580 Views
Human Immunodeficiency Virus - HIV Laboratory Testing. CLS 552 Application of Clinical Medical Microbiology & Immunology Karen Honeycutt, MEd , MLS(ASCP) CM SM CM. What is HIV?. H uman: infecting human beings

E N D
Human Immunodeficiency Virus - HIVLaboratory Testing CLS 552 Application of Clinical Medical Microbiology & Immunology Karen Honeycutt, MEd, MLS(ASCP)CMSMCM
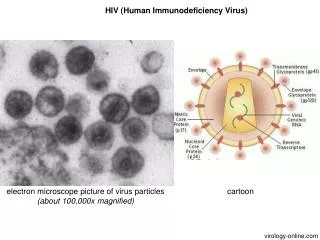
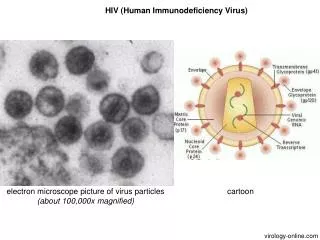
What is HIV? • Human: infecting human beings • Immunodefficiency: decrease or weakness in the body’s ability to fight off infections • Virus: a pathogen that only reproduces inside a living cell • RNA, single stranded, enveloped virus • Retrovirus: contains reverse transcriptase enzyme that converts RNA to DNA
Types of HIV • HIV 1 • Most common throughout the world • HIV 2 • Found in West Central Africa, parts of Europe and India • Both produce the same patterns of illness • HIV 2 disease progress slower than HIV 1
HIV Entry Into Cells • Viral envelope protein (gp 120) binds to target cells with CD4 receptor • CD4 T lymphocytes primary target cells • Other cells with CD4 receptor: • Macrophages • Peripheral blood monocytes • B lymphocytes (≈ 5%) • HIV turns host cell into HIV replication factory
How is HIV Transmitted • Unprotected sexual contact with infected partner • Exposure of broken skin to infected blood or body fluids • Transfusion with HIV infected blood products • Tissue transplantation • Injection with contaminated object • Mother to child during pregnancy, birth or breastfeeding • NOT by: saliva, respiratory droplets, insect vectors or close personal contact
Early Disease Progression ≈ 2-4 Weeks • HIV localizes in lymphoid organs • Viremia ensues after infection • Rapid spread within first few weeks after infection ≈ 30 billion virus particles produced in first weeks of infection • Acute retroviral syndrome: fever, fatigue, rash, headache, lymphadenopathy, pharyngitis, myalgias, nausea, vomiting, diarrhea, night sweats • Resolves in a few days to a few weeks
HIV Antibody Development • Detectable levels usually at 3 to 8 weeks after infection • Time between infection and detectable antibody levels = ‘window period’ • Serologic tests (looking for patient antibody) will be negative during window period • Viremia greatly decreased due to antibody • Patient usually asymptomatic • Clinical latency (average 10 years) • HIV continues to replicate in lymphoid tissue
Disease Progression • Severity of illness determined by: • Amount of virus in body • Degree of immune suppression: CD4 lymphocyte counts decrease • CD4 counts <500 usually become symptomatic, develop opportunistic infections
What is AIDS? • Acquired:come into possession of something new • Immune Deficiency: decrease or weakness in the body’s ability to fight off infections • Syndrome: signs and symptoms occurring together characterizing a particular abnormality AIDS is the final stage of the disease caused by infection with HIV.
Reasons for Testing for HIV • Identify those with infection so antiviral therapy can be initiated • Identify carriers who may transmit infection to others (blood & organ donors, pregnant women, sex partners) • Monitor disease progression • Evaluate treatment efficacy
Types of Testing • Most common • Serology to detect patient antibody production to HIV components • Nucleic acid testing (NAT) to detect HIV viral nucleic acid or characterize nucleic acid (resistance to antiviral drugs) • Less common • Detect HIV antigen (viral components) – usually used to screen blood products • Culture: very difficult and dangerous to perform
CDC Recommendation: Opt-Out Testing • Testing all persons aged13 to 64 years in all health care settings • Why? 250,000 in US unaware of HIV infection • Informed consent: inform patient HIV testing will be part of routine testing • Consent is inferred unless patient declines
Nebraska Law Requirements • Still requires patient signature indicating patient is consenting to HIV testing prior to blood being drawn • Bill in legislature (LB 462) to remove this restriction and follow CDC Opt-Out testing recommendations • Research indicates more patients consent to testing if seen as a routine test instead of a test to target at-risk behavior
Testing Algorithm – Standard SerologyPatient >2 years of age • Perform screening test • Enzyme immunoassay that will detect HIV antibodies in patient serum • Sensitivity and specificity ≈ 99% • Turn-around time = 1 to 2 days • If positive, the EIA test is repeated in duplicate on the same specimen • If 2 of 3 screen EIA tests are positive, confirmatory testing automatically performed
Testing Algorithm – Standard SerologyPatient >2 years of age • Confirmatory Testing – Western Blot • Viral components are separated via electrophoresis on nitrocellulose strips • Incubate patient serum with strips • If antibody present, antigen-antibody complexes form on strip • Strip is stained to visualize any antigen-antibody complexes • Positive: if 2 of 3 specific antigen-antibody bands present • Sensitivity & Specificity >99% • Turn-around time varies: 1-7 days
Testing Algorithm – Standard SerologyPatient >2 years of age • Confirmatory Testing – Western Blot Example + = positive control (-) = negative control pt. = patient • Patient WB = positive p24 and p120/160 bands present (Positive: if 2 of 3 specific antigen-antibody bands present) = Specific bands looked for
Testing Algorithm – Standard SerologyPatient >2 years of age • Patient is confirmed HIV positive if: • 2 of 3 screening tests are positive with confirmatory test (Western Blot) also positive • Test combination: >99% sensitive and >99.99% specific • If screen + and confirmatory negative, then patient is not considered positive: • Recommend follow up testing in 4 weeks • Reasons for false positive and false negative HIV serology (see next two slides)
Examples That Can Cause False Positive HIV Serology • Positive syphilis serology • Some malignant blood and autoimmune disorders • DNA viral infections • Alcoholic hepatitis • Chronic renal failure • Renal transplantation
Examples That Can Cause False Negative HIV Serology • Window period before seroconversion (most common) • Immunosuppressive therapy • Some malignancies • Bone marrow transplantation • Test systems that mainly detect antibodies to p24
HIV Point-of-Care Testing (POCT) • Public health needs for rapid HIV Tests • High rates of non-return for test results • Need for immediate information or referral for treatment choices • Perinatal settings • Post-exposure treatment settings • Screening in high-volume, high-prevalence settings
HIV Point-of-Care Testing (POCT) • Rapid or POCT is performed at the time the patient is seen clinically • Specimens: whole blood, saliva, urine • Only FDA approved assays used in health care settings • Results in 10-30 minutes • Sensitivity and specificity ≈ 99% • Considered a screen test • If positive confirmatory testing recommended • If negative usually no further testing recommended
HIV + Confirmed: Additional TestingQuantitative Plasma HIV RNA (Viral Load) • Not FDA approved for confirmatory testing as 2-9% false positive rate • Determine viral load ‘set point’ at time of diagnosis to monitor • patient disease progression • therapeutic response
HIV + Confirmed: Additional TestingCD4 Lymphocyte Count • Adult normal range = 700 to 1100 cells/mm3 • Results used to stage the disease • Make therapeutic decisions • When to start antiviral therapy • When to start prophylaxis for specific opportunistic infections • Indicator of prognosis
Perinatal HIV Infection in Infants • Utilize nucleic acid testing (NAT) • Can’t utilize serology as mother’s IgG HIV antibody will cross the placenta • Infant + if two HIV NATs positive at two different times • Early antiviral therapy is recommended in HIV + infants
Antiretroviral Therapy (2008) • HAART—highly active anti-retroviral therapy • 23 approved antiretroviral agents • Nucleoside Reverse Transcriptase Inhibitors • Non-NRTIs • Protease Inhibitors • Entry & Fusion Inhibitors • Integrase Inhibitors • 5 fixed dose combinations • Guidelines • DHHS—Department of Health and Human Services • IAS-USA—International AIDS Society - USA
Goals of HAART • Clinical: prolong life and improve quality of life • Virologic: undetectable viral load (<20-50 copies/mL) • Immunologic: immune reconstitution (normal CD4 count) • Therapeutic: combination of drugs (3 or 4) • Epidemiologic: reduce HIV transmission
Starting Antiretroviral Therapy • Start if: Patient symptomatic, an infant or pregnant HIV RNA >30,000 copies/ml CD4 count <350/mm3 • Consider if: HIV RNA <5000 copies/ml, CD4 count 350-500 /mm3 HIV RNA 5000-30000 copies/ml, CD4 count >500 /mm3 • Defer if: HIV RNA <5000 copies/ml, CD4 count >500 /mm3
Definition of Treatment Failure • Virologic failure Viral load not below detectable levels (>50-400 c/mL) • Side effects – patient not taking meds • Immunologic failure CD4 count fails to increase 100 cells/mm3 per year • Clinical failure >3 months post HAART and still having symptoms
HIV Resistance Testing • Genotypic testing: HIV gene sequencing of the patient’s virus to detect mutations known to confer drug resistance • Report out specific gene sequences with the drugs that the virus will be resistant to • Reasons to perform • When patient is first diagnosed as baseline • At the start of HAART or switching drugs • Determine if patient has been infected with other virus strains • Treatment failures
Opportunistic Infections • Pneumocystisjiroveci(carinii) - fungi • Causes pneumonia (PCP) • Detection via stains of BAL fluid, lung tissue • Mycobacterium tuberculosis • Lung and systemic disease • Detection via culture • Mycobacterium aviumcomplex (MAC) • Disseminated disease • Detection via culture
Opportunistic Infections • Cryptosporidium sp. - parasite • Diarrhea • Detection of organism is stool via microscopy or antigen detection • Toxoplasmagondii- parasite • Encephalitis, brain abscess • Detection via serology (looking for antibody), staining tissue or NAT
Opportunistic Infections • Candida sp. - yeast • Thrush, vaginitis, esophagitis • Detection with culture • Cryptococcus neoformans- yeast • Meningitis, pneumonia, disseminated disease • Detection via culture or antigen detection in CSF • Cytomegalovirus (CMV) • Retinitis, pneumonia • Detection via viral culture, NAT
Summary • HIV: single-stranded, RNA, enveloped, retrovirus • Infect CD4 positive cells: especially CD4 lymphocytes • Serology: 2 of 3 screen tests positive followed by positive confirmatory test = HIV + • Monitor: CD4 count, viral load, resistance testing • CD4 count <500 = possible opportunistic infections <350 = probably initiate antiviral therapy