Download
1 / 40
400 likes | 616 Views
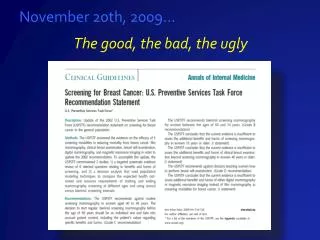
November 20th, 2009… The good, the bad, the ugly. The USPSTF recommends against routine screening mammography in women aged 40-49.

E N D
November 20th, 2009… The good, the bad, the ugly
The USPSTF recommends against routine screening mammography in women aged 40-49. The decision to start…should be an individualized one and take patient context into account, including the patients values regarding specific benefits and harms.” (C recommendation) Moderate certainty that the net benefit is small Annals of Int. Med Nov. 2009: 151 (10) 716-726
Additional USPSTF recommendations… Women 50 – 74 yrs: change from every 1-2 yrs to every 2 yrs • Insufficient evidence for or against screening women after 75 yrs Insufficient evidence for or against CBE in women > 40 yrs Recommended against physicians teaching BSE Annals of Int. Med Nov. 2009: 151 (10) 716-726
What was “good”? Evidence-based guidelines are critical for medical decision making • Outcome data should representative “real world” scenarios • USPSTF used Breast Cancer Surveillance Consortium (BCSC) data representing a mix of breast imaging practices • academic, private, geographically diverse
What was “bad”? The presentation…
By GINA KOLATA Published: November 21, 2009 The current dispute over mammograms gives many people who’ve been around since the 1980s a sense of déjà vu. Like archeologists arguing endlessly over the same set of bones, cancer specialists, it can seem, have been arguing endlessly over pretty much the same set of data….. Get a Mammogram. No Don’t. Repeat.
What was “ugly”? Data on which analyses were based was old (same RCTsfrom 1980’s - 2002 used in prior USPSTF recs) • Mortality reductions significantly less than newer trials • False positive rates higher • Radiation risk overestimated • BCSC data from pre-digital mammo era (<2005) Why wasn’t newer data used?
Outcomes Table Annals of Int. Med Nov. 2009: 151 (10) 716-726
Diagnostic Performance of Digital versus Film Mammography for Breast-Cancer ScreeningEtta D. Pisano, M.D., Constantine Gatsonis, Ph.D., Edward Hendrick, Ph.D., Martin Yaffe, Ph.D., Janet K. Baum, M.D., Suddhasatta Acharyya, Ph.D., Emily F. Conant, M.D., Laurie L. Fajardo, M.D., Lawrence Bassett, M.D., Carl D'Orsi, M.D., Roberta Jong, M.D., Murray Rebner, M.D., for the Digital Mammographic Imaging ScreeningTrial (DMIST) Investigators Group Published at www.nejm.org September 16, 2005 Diagnostic Performance of Digital versus Film Mammography for Breast-Cancer ScreeningEtta D. Pisano, M.D., Constantine Gatsonis, Ph.D., Edward Hendrick, Ph.D., Martin Yaffe, Ph.D., Janet K. Baum, M.D., Suddhasatta Acharyya, Ph.D., Emily F. Conant, M.D., Laurie L. Fajardo, M.D., Lawrence Bassett, M.D., Carl D'Orsi, M.D., Roberta Jong, M.D., Murray Rebner, M.D., for the Digital Mammographic Imaging ScreeningTrial (DMIST) Investigators Group Published at www.nejm.org September 16, 2005
ACRIN Digital Trial 6652 - DMIST 33.1% 21.5% 78.6% 64.9% 72 cancer in 14,130 women = 5.1 cancers/1000 in women < 50 years
Non- Randomized Controlled Trial Journal of Cancer Cancer: Aug. 1, 2002/Vol 95/No. 3 The Impact of Organized Mammography Service Screening on Breast Carcinoma Mortality in Seven Swedish Counties A Collaborative Evaluation Stephen W.Duffy, Msc., Laszlo Tabar, M.D. Hsui-His Chen, D.D.S.Ph.D., Marit Holmqvist Ming-Fang Yen, M.Sc.,et al. Background: The evaluation of organized mammographic service screening programs is a major challenge in public health. In particular, there is a need to evaluate the effect of the screening program on the mortality of breast carcinoma, uncontaminated in the screening epoch by mortality from 1) cases diagnosed in the prescreening period and 2) cases diagnosed among unscreened women (i.e., nonattenders) after the initiation of organized screening.
Cancer: Aug. 1, 2002/Vol 95/No. 3 Method:Population based screen program begun in 1978-89 • Screening performed every 1.5 - 2 years. Conclusions:Death rate in Swedish Seven Counties decreased over past 29 yrs in proportion to % women screened • For screened women: • Death rate decreased by 44% For those refusing screening, no change in death rate
Journal of Cancer Effectiveness of Population-Based Service Screening With Mammography for Women Ages 40 to 49 Years Barbro Numan Hellquist, MSc1; Stephen W. Duffy, MSc2; Shahin Abdsaleh, MD, PhD3; Lena Bjo¨rneld, RN4; Pa´l Borda´s, MD5; La´szlo´ Taba´r, MD, PhD6; Bedrich Vita´k, MD, PhD7; Sophia Zackrisson, MD, PhD8; Lennarth Nystro¨m, PhD9; and Ha˚kan Jonsson, PhD1 RESULTS: There was no significant difference in breast cancer mortality during the prescreening period. During the study period, there were 803 breast cancer deaths in the study group (7.3 million person-years) and 1238 breast cancer deaths in the control group (8.8 million person-years). The average follow-up was 16 years. The estimated RR for women who were invited to screening was 0.74 (95% CI, 0.66-0.83), and the RR for women who attended screening was 0.71 (95% CI, 0.62-0.80). CONCLUSIONS: In this comprehensive study, mammography screening for women ages 40 to 49 years was efficient for reducing breast cancer mortality. Cancer: online publication 9/29/10
Swedish Screening Update 2011 Methods: • Women aged 40 -49 yrsinvited to screen vs those not invited • Outcome measure breast CA death • The average follow-up 16 years (1986 to 2005) Results: • 803 deaths in study group (7.3 million person-years) • 1238 deaths in control group (8.8 million person-years) • RR for those invited to screen was 0.74 (95% CI, 0.66-0.83) • RR for those attended screening was 0.71 (95% CI, 0.62-0.80) Those who actually participated in screening had 29% lower BCA mortality than those who were not invited to screening
Woman screened to prevent 1 death? Estimate of 1904 women in 40’s needed to be invited to screening to prevent 1 BCA death is way off... • Using newer data from women actually screened and followed for 20 yrs, NNI was 726 This number is even less that what was estimated by USPSTF for women in 50’s (1339)
What about Risks? Yes, mammography is far from perfect and the risk of a false positive is ~50% with decade of routine screening • What are false positives? • 10% call back rate from screening • Approx. 2.4% biopsy rate (24/1000) Nevertheless, women report they would accept trade-off of FP in favor of finding cancer early1 Schwartz LM et al. BMJ 2000;1635-40.
Cancer diagnosed in 40’s? Cancers that occur in pre-menopausal women have a more rapid growth rate • One in 6 breast cancer deaths are attributable to women diagnosed in their 40’s • One third of all years lost to breast cancer deaths are due to women diagnosed in their 40’s Wu LC et al. Ann Inten Med 2012;157;597. Shapiro S et al. HIPP and Sequelae, JHU Press 1988
Perspective: • United States Preventive Services Task Force Screening Mammography Recommendations: Science Ignored • R. Edward Hendrick1 and Mark A. Helvie21 • Objective: To examine the scientific evidenceused by USPSTF to recommendagainst screening mammography: • Women 40–49 yearsold • Against annual screening mammography in women 50 andolder. AJR 2011; 196:W112-W116
Conclusions Averaged over six USPSTF models of benefit for annual screening: • For 40–74 yrs: up to 39.6% mortality reduction • 71% more lives saved than USPSTF biennial screening for 50–74 yrs olds, which had 23.2% mortality reduction For 40–84 years: 99,829 more lives saved than USPSTF recs ifall women comply, and 64,889 more lives with the current 65%compliance rate AJR 2011; 196:W112-W116
Potential Harms? For screening women 40–49 yrs screened yearly? • a recall for diagnostic workup every 12 years • a negativebiopsy every 149 years • a missed breast cancer every 1,000 years • anda fatal radiation-induced breast cancer every 76,000–97,000years “Evidence made available to USPSTF strongly supportsthe mortality benefit of annual screening mammo beginningat age 40 yrs, whereas potential harms of screening with thisregimen are minor” AJR 2011; 196:W112-W116
The Screening Process General Population Populationwith Disease
Risk Stratification • Gender • Personal/Family History • Exposure history • Genetics • Serum Biomarkers • Tissue Markers from Prior Biopsy • Risk Models (Claus/Gail) Imaging --- what quantitative measures can we use?
Density as a Risk Factor Mammographic dense tissue, percent densearea (PD) is one of strongest risk factors for breast cancer Boyd et al., NEJM 2007
Women with >50% dense breasts are at 3- to 5X greater risk for breast cancer than women with density <25%2 • Partly due to the lower sensitivity of mammo but remains even when accounting for “masking” • Mammo dense breast tissue is rich in epithelium and stroma and association could represent activation of these cells Mammographically dense breast tissue results in up to 3X higher false positive call-backs at screening3 Boyd 1995, 2Tice Ann Intern Med. 2008, 3Yankaskas AJR 2001
Breast Density Estimation Cumulus (Univ. Toronto) PD = 42.5%
Annals of Internal Medicine Established in 1927 by the American College of Physicians Using Clinical Factors and Mammographic Breast Density to Estimate Breast Cancer Risk: Development and Validation of a New Predictive Model Jeffrey A. Tice, MD; Steven R. Cummings, MD; Rebecca Smith-Bindman, MD; Laura Ichikawa, MS; William E. Barlow, PhD; and Karla Kerlikowske, MD Conclusion: A breast cancer prediction model that incorporates routinely reported measures of breast density can estimate 5-year risk for invasive breast cancer. Its accuracy needs to be further evaluated in independent populations before it can be recommended for clinical use. Ann Intern Med. 2008;148:337-347
Computer-Assisted Risk Estimation General Population Risk stratification Image assessment Image Screening Imaging diagnosis/guided biopsy Population with Disease Identify women at high risk of breast cancer, so customized screening protocols and individualized risk reduction strategies may be implemented
Patient questionnaire Calculated glandularity Tailored screening recommendations
What about DCIS? In U.S. in 1983 (prescreening era) 4,900 women were diagnosed with DCIS In 2010, approximately 54,000 women who will be diagnosed with DCIS (20-30% of cancers diagnosed) How do we tell the bad actors from the less bad ones??? http://www.seer.cancer.gov/csr/1975_2007/browse_csr.php?section=4&page=sect_04_zfig.01.html
Graph shows age-adjusted incidence rates of DCIS in the United States from 1975 to 2007. Jørgensen K J et al. Radiology 2011;260:621-627