Download
1 / 8
80 likes | 204 Views
This document reviews crucial recommendations regarding Stage 2 Meaningful Use (MU) for EHR reporting and Clinical Quality Measures (CQMs). It suggests a 90-day continuous reporting period for the first year and a 365-day period for subsequent years. There is concern about the feasibility of menu options and the accountability of providers for patient actions. The recommendations emphasize that CMS should assess the feasibility of measures, allow flexibility in reporting, and reduce the total number of CQMs, while ensuring alignment with measure steward programs.

E N D
MU Stage 2 Comments EHR Reporting Period • There will be a short window of time between final rule and Oct. 1, 2013 where developers will have to create, test and certify technology and providers will have to implement and train users • While Stage 2 does not start from scratch, there are many new functions and processes expected • Recommendation: Continuous 90-day reporting period within first year of Stage 2; 365-day reporting period for subsequent years within the same stage “All Patients” Denominator • Majority of patients will have EHRs by 2014, not all patients • Difficult for CMS to audit whether an EP’s or hospital’s data actually included the provider’s entire population • Recommendation: Continue Stage 1 policy of allowing for a mix of measure denominators, not a single “all patient”
MU Stage 2 Comments Core and Menu Sets • Compliment CMS for continuing core and menu approach • Worry that there are too few menu options • Many providers will find it difficult to achieve 2 of 4 (hospitals) or 3 of 5 (EPs) • Some of the menu options will require significant investment • Recommendation: CMS needs to carefully assess the feasibility of each menu option to make sure the average provider will be able to meet reasonable objectives. This, in turn, may necessitate more menu options (we later suggest which core objectives could move to menu)
MU Stage 2 Comments View Online, Download or Transmit • The CMS approach of requiring measurement of patient use is flawed • Providers should not be held accountable for the actions or inactions of third parties, especially when inaction may be due to a wide range of reasons • Recommendation: CMS first investigate the underlying need for requirements listed in measure (B). If CMS is confident that download and transmit options are widely used by patients, we believe measure (B) could simply require the capability for patients to view online, download and transmit their health information, but not make providers liable for patient use of these capabilities. • Content standards for “care team members” “providers of care” and “goals” contained within the Consolidated CDA need more definition – it is unclear what providers are accountable for and how CMS will audit these fields • Recommendation: Continue use of CCD content standards for this and other measures/objectives
MU Stage 2 Comments Transitions of Care - Two measures (A) 65 percent of Summary of Care records are electronic • A lower threshold would recognize that large numbers of potential recipients may not be prepared or willing to accept a summary care record electronically (B) 10 percent of SoC records are sent electronically between two unaffiliated providers who use different systems • We oppose measure (B) based on potential workflow issues, patient safety issues and a general question of feasibility. • We recognize that this measure is intended to increase interoperability and, more generally, make it easier for providers to communicate with one another. • Recommendation: We propose a voluntary reporting concept that would be similar to error reporting found on all major operating systems used in desktop or laptop computing. If a provider submits a summary care record and is unable to do so because the system has been implemented in a way that prohibits or limits communication, an error report could be sent to ONC and CMS in the same way error reports are sent to Microsoft. • CHIME believes this kind of approach would mitigate many unintended consequences and reduce the number of needed exclusions, while pushing forward the goal of interoperability.
MU Stage 2 Comments Clinical Quality Measures – Reporting Period • Most organizations do not have the resources to invest in positioning themselves for future changes in technology, including CQM reporting tools, without a hard target or objective. • Recommendation: To follow-up on recommendations made earlier, we would like to reiterate our view that CMS should adopt a 90-day continuous CQM reporting period for the first year of Stage 2 to mirror that of the EHR reporting period.
MU Stage 2 Comments Clinical Quality Measures • Recommendation: CHIME believes that CMS needs to reduce the total number of CQMs if they keep the current mix of domains and CQMs. While we support the direction CMS is taking with the domains, we believe some domains lack a sufficient number of CQM options. For this reason, we are asking that CMS reduce the total number of CQMs that hospitals have to report to 15 – 18 CQMs. • Recommendation: To follow-up on recommendations made earlier, we would like to reiterate our view that CMS should adopt a 90-day continuous CQM reporting period for the first year of Stage 2 to mirror that of the EHR reporting period. • Recommendation: The Meaningful Use specifications for clinical quality measures should be in line with the measure steward programs’ specifications, so EHR vendors do not need to develop and maintain two versions of the same metric.
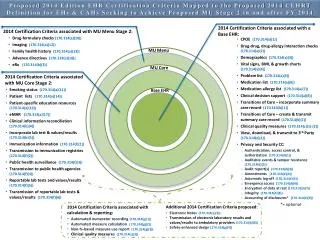
MU Stage 2 Comments Standards & Certification – CEHRT definition • We understand the CEHRT definition would apply both Stage 1 and Stage 2 beginning FY / CY 2014, but we are concerned this approach may lead to higher costs and increased complexity for some providers. • If providers purchase technology based on the 2011 Edition in FY / CY 2013 – before 2014 Edition technology is available – we fear they will incur time loss and expenses to upgrade the year immediately after initial implementation. • Recommendation: We propose that ONC allow use of the 2011 Edition CEHRT until FY / CY 2015, so that all Meaningful Use participants have equal opportunity to spend two years with the same or similar technology
MU Stage 2 Comments Standards & Certification – “at least one” provision • Past experience is mixed on the assumption that “EHR technology developers would design EHR technology to incorporate the data elements for, and calculate, those CQMs they believe their EHR technology would need to include in order to support the providers to which they market their EHR technology.” As previously stated in this letter, and recognized by ONC in their Stage 2 NPRM, some vendors chose to certify only the minimum required number of CQMs in Stage 1, irrespective of provider quality measure priorities. • The Base EHR is the only component of the three-piece 2014 Edition where CQM certification criteria are addressed. • Recommendation: As part of Base EHR certification, we propose that ONC require certification to all CQMs needed to meet Meaningful Use in each setting. CHIME believes that certification should include all CQMs for associated settings. And in order to minimize the costs of development and implementation, we recommend that ONC work with CMS to limit the total number of CQMs associated with each setting. • Recommendation: As an alternative approach, CHIME recommends that ONC divorce CQMs from the Base EHR definition and make CQMs a standalone Module that can be tied to other setting-specific criteria, such as the MU Core or MU Menu pieces of the 2014 Edition.