Download
1 / 78
780 likes | 933 Views
Understanding Stage 2 MU. Core & Menu Objectives. EHR Incentives. The Medicare EHR Incentive program provides incentive payments to EPs as they adopt , implement, upgrade or demonstrate meaningful use of certified EHR technology .

E N D
Understanding Stage 2 MU Core & Menu Objectives
EHR Incentives • The Medicare EHR Incentive program provides incentive payments to EPs as they adopt, implement, upgrade or demonstrate meaningful use of certified EHR technology. • Eligible professionals can receive up to $44,000 over five years • Participation began in 2011. • Starting in 2015, Medicare EPs that do not demonstrate meaningful use will have a payment adjustment
The money is real I received $18,000 in 2012 (from 2011) *deposit after taking out a little for myself
The money is real I received $12,000 in 2013 (from 2012) *I should have taken out a little for myself
Meaningful Use • Providers have to show that they are “meaningfully using” their EHRs by meeting thresholds for a number of objectives. • Staged in three steps with increasing requirements for participation. • All providers begin by meeting Stage 1 for a 90-day period in their first year and a full year in their second year • After meeting Stage 1, providers will then have to meet Stage 2 requirements for two full years.
Full Timeline * Only 90 Days of MU Required in 2014
Stage 2 & 3 Delayed • Stage 2 extended through 2016 • Stage 3 starts in 2017 • for providers who have completed at least two years of the prior level of EHR adoption.
Stage 2 Timeline • In the Stage 1, CMS had established a timeline that required providers to progress to Stage 2 criteria after two program years. • However, CMS had delayed the onset of Stage 2 criteria until 2014
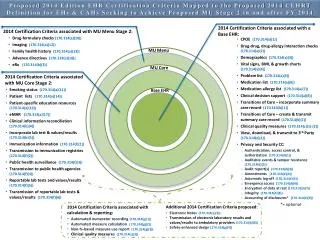
Overview of Changes Stage 1 Stage 2 17 Core Objectives 6Menu Objectives Must complete 3 All 3 are EPs choice 9 CQMS 3 Core Other 6 are EPs choice • 15 Core Objectives • 10 Menu Objectives • Must complete 5 • 1 must be public health • Other 4 are EPs choice • 6 CQMS • 44 Total • 3 Core • Other 3 are EPs choice
New Objectives & Measures • Most of the new objectives introduced for Stage 2 are menu objectives • EPs have a new core objective that they must achieve. • CMS believes that this objectives will have a positive impact on patient care and safety • New Stage 2 Core Objectives: • Use secure electronic messaging to communicate with patients on relevant health information
Replaced Objectives • Stage 2 also replaces the previous Stage 1 objectives: • provide electronic copies of health information and (Stage 1 Core 12) • provide timely access to health information with objectives that allow patients to access their health information online. (Stage 1 Menu 5) • With the new Stage 2 objective • Provide patients the ability to view online, download and transmit health information within four business days of information being available to the EP
Increased Emphasis on HIE • One of the core objectives requires EPs who transition or refer a patient to provide a summary of care record for more than 50% of those transitions of care and referrals. • For more than 10% of transitions EPs must provide a summary of care electronically. • Must either a) conduct successful electronic exchanges with a recipient using different EHR technology, OR b) conduct successful tests with the CMS-designated test EHR
Requires patient participation • New Stage 2 measures for several objectives that require patients to use health information technology • Core 7: Provide patients the ability to view online, download and transmit their health information. More than 5% of patients must do so. • Core 17: Use secure electronic messaging to communicate with patients on relevant health information. More than 5% of patients must do so
Overview of Changes Stage 1 Stage 2 17 Core Objectives 6Menu Objectives Must complete 3 All 3 are EPs choice 9 CQMS 3 Core Other 6 are EPs choice • 15 Core Objectives • 10 Menu Objectives • Must complete 5 • 1 must be public health • Other 4 are EPs choice • 6 CQMS • 44 Total • 3 Core • Other 3 are EPs choice
Core 1: CPOE Stage 1 Stage 2 Use computerized provider order entry (CPOE) for medication, laboratory and radiology orders 60% for meds (30% for labs and radiology) • Use computerized provider order entry for medications • 30%
Core 1: CPOE • Radiology Order – Order for any imaging services that uses electronic product radiation. The EP can include orders for other types of imaging services that do not rely on electronic product radiation in this definition as long the policy is consistent across all patient and for the entire EHR reporting period. • Electronic Product Radiation – Any ionizing or nonionizing electromagnetic or particulate radiation, or [a]ny sonic, infrasonic, or ultrasonic wave that is emitted from an electronic product as the result of the operation of an electronic circuit in such product.
Core 1: CPOE • Made up of 3 measures • Medications • Radiology • OCT • Pachymetry • Optos • Laboratory • Exclusion - Any EP who writes fewer than 100 medication, radiology, or laboratory orders during the EHR reporting period.
Core 2: Electronic prescribing Stage 1 Stage 2 More than 50% prescriptions written are transmitted electronically And compared to at least one drug formulary • More than 40% prescriptions written are transmitted electronically using certified EHR technology
Core 2: Electronic prescribing • Exclusion for any EP who: • Writes fewer than 100 permissible prescriptions during the EHR reporting period. • Does not have a pharmacy that accept electronic prescriptions within 10 miles of the EP's practice location
Core 3: Demographics Stage 1 Stage 2 More than 80% of all unique patients seen by the EP have demographics recorded as structured data • More than 50% of all unique patients seen by the EP have demographics recorded as structured data
Core 3: Demographics • Required Demographics • Preferred language • Gender • Race • Ethnicity • Date of birth • Exclusion - none
Core 4: Vital Signs Stage 1 Stage 2 More than 80% of all unique patients Age 3 and over blood pressure All ages height and weight recorded as structured data • For more than 50% of all unique patients • Age 2 and over blood pressure, height and weight are • recorded as structured data
Core 4: Vital Signs • Vital sign information can be entered into the patient's medical record in a number of ways including: direct entry by the EP; entry by a designated individual from the EP’s staff; data transfer from another provider electronically, through an HIE or through other methods; or data entered directly by the patient through a portal or other means. Some of these methods are more accurate than others, and it is up to the EP to determine the level of accuracy needed to care for their patient and how best to obtain this information.
Core 4: Vital Signs • Exclusion - any EP who: • Sees no patients 3 years • Believes that all 3 vital signs have no relevance to their scope of practice • Believes that but blood pressure is not • Believes that height/length and weight are not • Does not have to be updated at every patient encounter
Core 5: Smoking Status Stage 1 Stage 2 Record smoking status for 80% of patients 13 years old or older • Record smoking status for 50% of patients 13 years old or older
Core 5: Smoking Status • Exclusion - Any EP that neither sees nor admits any patients 13 years old or older.
Core 6: Clinical decision support Stage 1 Stage 2 Implement 5 clinical decision support interventions related to 4 or more clinical quality measures, Enabled drug-drug and drug-allergy interaction checks • Implement one clinical decision support rule relevant to specialty or high clinical priority
Core 6: Clinical decision support • CMS will not issue additional guidance on the selection of appropriate clinical decision support rules for Stage 2 Meaningful Use. This determination is best left to the EP taking into account their workflow, patient population, and quality improvement efforts.
Core 7: Patient online access Stage 1 Stage 2 More than 50% of patients seen are provided timely (4 business days) online access to their health information More than 5% view, download, or transmit to a third party their health information • Provide patients with an electronic copy of their health information upon request
Core 7: Patient online access • Information that must be made available online: • Patient name • Provider's name and office contact information • Current and past problem list • Procedures • Laboratory test results • Current medication list and medication history • Current medication allergy list and history • Vital signs • Smoking status • Demographic information • Care plan field(s) including goals and instructions • Any known care team members including the primary care provider
Core 8: Clinical summaries Stage 1 Stage 2 Clinical summaries provided to patients for more than 50% of office visits within one business day • Clinical summaries provided to patients for more than 50% of all office visits within 3 business days
Core 8: Clinical summaries • Can be provided through a PHR, patient portal on the web site, secure e-mail, electronic media such as CD or USB fob, or printed copy. • Where there is no information available to populate one or more of the fields, either because the EP can be excluded or because there is no information to record an indication that the information is not available would meet the measure
Core 9: Protect ehealth info Stage 1 Stage 2 Conduct or review a security risk analysis per 45 CFR 164.308 (a)(1), including addressing the encryption/security of data at rest implement security updates as necessary correct identified security deficiencies as part of its risk management process • Conduct or review a security risk analysis per 45 CFR 164.308 (a)(1) • implement security updates as necessary • correct identified security deficiencies as part of its risk management process
Core 9: Protect ehealth info • No exclusion • EPs must conduct or review a security risk analysis of CEHRT including addressing encryption/security of data, • The parameters of the security risk analysis are defined 45 CFR 164.308(a)(1) which was created by the HIPAA Security Rule.
Core 10: Incorporate test results Stage 1 Stage 2 Incorporate more than 55%clinical lab-test results into Certified EHR technology as structured data • Incorporate more than 40%clinical lab-test results into Certified EHR technology as structured data
Core 10: Incorporate test results • Exclusion - any EP who orders no lab tests where results are either in a positive/negative affirmation or numeric format during the EHR reporting period. • Lab results are not limited to any specific type of laboratory or to any specific type of lab test.
Core 11: Patient lists Stage 1 Stage 2 Generate lists of patients by specific conditions to use for quality improvement, reduction of disparities, research, or outreach • Generate lists of patients by specific conditions to use for quality improvement, reduction of disparities, research, or outreach
Core 11: Patient lists • Enable a user to electronically and dynamically select, sort, access, and create patient lists by: date and time; and based on each one and at least one combination of the following data: • Problems; • Medications; • Medication allergies; • Demographics; • Laboratory tests and values/results; and • Ambulatory setting only -Patient communication preferences.
Core 12: Provide reminders Stage 1 Stage 2 Use EHR to identify and provide reminders for preventive / follow-up care for more than 10% of patients with two or more office visits in the last 2 years Core item • Use EHR to identify and provide reminders for preventive / follow-up care for 20% of all unique patients 65 years or older or 5 years old or younger • Was a menu item
Core 12: Provide reminders • Additional information: • per patient preference when available. • such as (but not limited to) by mail, by phone or by secure messaging. • Reminders must be sent using the preferred communication medium only when it is known by the provider. • To count for the measure, reminders for preventive/follow-up care must be for care that the patient is not already scheduled to receive
Core 13: Patient education Stage 1 Stage 2 Use certified EHR technology to identify patient-specific education resources 10% of patients Core Item • Use certified EHR technology to identify patient-specific education resources • 10% of patients • Was a menu item
Core 13: Patient education • While CEHRT must be used to identify patient-specific education resources, these resources or materials do not have to be stored within or generated by the CEHRT. • electronic copy, • printed copy, • electronic link to source materials, • through a patient portal or PHR
Core 14: Med reconciliation Stage 1 Stage 2 Perform medication reconciliation for more than 50% of transitions of care to the care of the EP Core item • Perform medication reconciliation for more than 50% of transitions of care to the care of the EP • Menu item
Core 14: Med reconciliation • Medication Reconciliation - The process of identifying the most accurate list of all medications that the patient is taking, including name, dosage, frequency, and route, by comparing the medical record to an external list of medications obtained from a patient, hospital, or other provider. • The electronic exchange of information is not a requirement for medication reconciliation.