Download
1 / 24
240 likes | 1.12k Views
CT diagnosis of malpositioned chest tube. Intern 劉一璋. Abstract (1). Insertion of a chest tube into the pleural space is standard management for various pleural disorders. Malpositioning of chest tubes in extrathoracic , intraparenchymal and

E N D
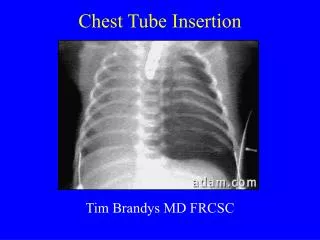
CT diagnosis of malpositioned chest tube Intern 劉一璋
Abstract (1) • Insertion of a chest tube into the pleural space is standard management for various pleural disorders. • Malpositioning of chest tubes in extrathoracic, intraparenchymal and mediastinal locations and in the fissures is common. • Malpositioning results not only in inadequate drainage of air and fluid but may also result in increased morbidity and mortality.
Abstract (2) • Diagnosis of a malpositioned tube is sometimes difficult to establish on a chest radiograph. • CT, however, has proven to be extremely accurate in evaluating the position of a chest tube and has often provided additional valuable information with significant therapeutic impact.
Indication for chest tube insertion • pneumothorax, • penetrating chest injuries, • haemothorax, • empyema, • bronchopleural fistula
Optimal tube placement • for fluid drainage: a dependent location at the posterior base • for air evacuation: a non-dependent position is preferred, apical and anterior
Risk of malpositioned chest tube • Malpositioning of chest tubes is common, especially in traumatic chest injury. • Malpositioning not only results in inadequate drainage of air and fluid but also increased morbidity and mortality. • Usually require immediate repositioning or replacement.
Diagnosis of a malpositioned tube • is sometimes difficult to establish because: (1) clinical manifestations may be absent (2) a bed-side chest radiograph is usually unreliable in demonstrating the exact location of the tube
Diagnosis of a malpositioned tube • CT (1) is extremely accurate in evaluating the position of a chest tube (2) often provides additional valuable information with significant therapeutic impact. • The aim of this pictorial review is to provide an overview of malpositioned chest tubes diagnosed on CT.
Recognition of malpositioned chest tubes on CT • CT is indicated: (1) when a chest tube does not drain adequately (2) the chest radiograph is non-contributory.
CT for malpositioned chest tubes • Different window settings are necessary. • pulmonary and pleural lesions may conceal the course of the tube on a lung window. • A bone window may be of advantage in an extrapleural tube location, where its attenuation may be similar to that of the ribs. • In addition, thin sections in a lung window setting may clarify whether a tube is intrafissural or intraparenchymal.
Intraparenchymal tube placement • is most likely to occur with pre-existing pulmonary disease or pleural adhesions. • On CT, the tube is seen traversing the lung. • Probably representing a haematoma due to lung laceration. • A parenchymal tract may sometimes remain after removal of a tube. • A chronic bronchopleural fistula or lung abscess may also result
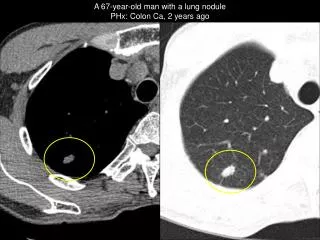
CT shows the tube is intraparenchymal and does notreach the loculated anterior pneumothorax.
CT (mediastinal window) demonstrates a tube entering through the left anterior chest wall, coursing posteriorly in the apex of the left lung. Lung window: Increased attenuation of the lung parenchyma surrounding the tube is probably haematoma
Intrafissural tube placement • A chest tube is considered to be intrafissural (1) when it is outlined by a residual pneumothorax (2) when it is located in the region of a fssure but without areas of an intraparenchymal opacity around it.
Chest CT (mediastinal window), contiguous sections at the lung base show the right tube within the oblique fissure, crossing the hemithorax, with its tip very close to the dilated contrast-filled oesophagus.
Mediastinal tube placemen • A tube that has been introduced too far into the thorax may reach the mediastinum. • On CT, the position of the tube can easily be seen abutting the mediastinum. • Reported complications include: perforation of the heart, the pulmonary artery and the esophagus.
A 3.5-year-old girl with a right pleural effusion and a lung infiltrate. • A tube was inserted into the right hemithorax. • Chest CT (lung window): • a right hydropneumothorax is present. Part of the tube is seen anteriorly; • its tip cannot be accurately defined. • (b) Chest CT (mediastinal window, same level as (a)): • again the tip of the tube is not well visualized owing to artefacts from a metallic device on the left chest wall, but it probably • abuts the superior vena cava and the ascending aorta.
Chest wall tube placement • When a tube tip is positioned outside the parietal pleura it is considered to be in the chest wall. • Inserting the tube too cranially and too medially may cause bleeding from the pectoralis major muscle, especially in men, and may damage the breast in women. • High insertion in the posterior chest wall has resulted in Horner's syndrome.
The tip of a left chest tube lies in the left lateral chest wall (arrow).
A gunshot wound at the level of D3 in a29-year-old man. CT demonstrates bilateral pneumothoraces. A tube has been inserted anteriorly to drain the left pneumothorax, causing a haematoma in the pectoralis major muscle (asterisk).
Abdominal placement of a chest tube • When the tube is placed too low it may enter the peritoneal cavity and can be seen on CT with the tip below the diaphragm. • The spleen and liver have been injured most commonly in such cases. • Gastric injury from a trocar has also been reported.
On CT: The lower tube is seen entering the lateral aspect of the spleen (arrow). A tube is seen traversing the left costophrenic angle (arrow).
A 36-year-old woman with bilateral pleural effusions and pneumonia. CT was performed because of a drastic drop of haemoglobin. Chest CT (mediastinal window) at level of diaphragm shows: a right pleural effusion posterior to an atelectatic segment of the right lower lobe. The lateral aspect of the liver is surrounded by fluid of high density. Air bubbles within the peritoneal fluid indicate an intra-abdominal placement of the tube. A left tube had been inserted earlier to drain the left pleural effusion.