Download
1 / 32
860 likes | 4.32k Views
Chest Tube Insertion and Needle Decompression. AFAMS Resident Orientation April 8, 2012. Outline. Needle Decompression Chest Tube Insertion Indications / Contraindications Equipment Insertion Confirming Placement Managing Chest Tubes Toubleshooting.

E N D
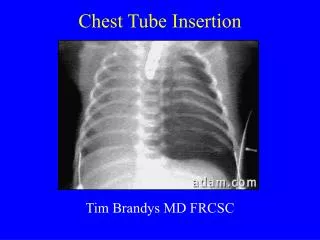
Chest Tube Insertion and Needle Decompression AFAMS Resident Orientation April 8, 2012
Outline • Needle Decompression • Chest Tube Insertion • Indications / Contraindications • Equipment • Insertion • Confirming Placement • Managing Chest Tubes • Toubleshooting
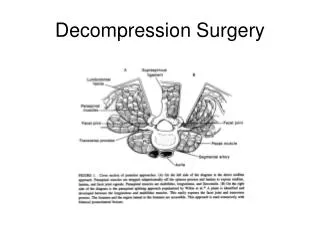
Needle Decompression Indications دیکمپریشن پلورا • Emergency Use for Tension Pneumothorax • Not indicated for simple pneumothorax, open pneumothorax or flail chest • If done in a patient without pneumothorax, increased morbidity • موارداستفاده • - کمک عاجل برای تنشن نموتوراکس • نوت درحالاتی که مریض نموتوراکس ساده، نموتوراکس باز،هیموتوراکس یا flail chest داشته باشد موثرواقع نمی ش
Tension Pneumothorax تنشن نموتوراکس Signs and Symptoms اعراض وعلایم صدای تنفس موجود نمی باشد یا تقلیل میابد بلند شدن صدربه شکل غیرمساویانه Dyspnea افزایش میابد ناراحتی / اضطراب نشانه ها یا تاریخچه جرحه غشای صدر وریدهای عنق متورم میگردد ضعیف شدن یا کم عرض شدن فشارنبض شاک mediastinal shift (late) • Decreased or low breath sounds • Unequal chest rise • Dyspnea increases • Discomfort/anxiety • Signs and history of chest injury • Jugular veins inflated • Weakness of pulse pressure • Shock • Mediastinal shift (late)
Locations for Needle Decompressionانتخاب ناحیه • Preferred • 2nd or 3rdintercostal space, mid clavicular line • Alternative • 5thintercostal space, mid axillary line • For patient transportation, other sites are not recommended. • Always place needle above the rib! • ترجیح داده شده • جوف دوم یا سوم بین الضلعی ، خط وسطclavicular • الترنیتو • جوف بین الضلعی پنجم ، خط وسط axillary • برای انتقال دادن مریض ، ناحیه های دیگر توصیه نمی گردد
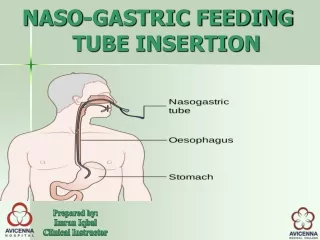
Chest Tubeچست تیوب Indications موارد استعمال و هدف دریناژ مایع و هوا ازجوف پلورا یا mediastinum برای تداوی نموتوراکس ، هیموتوراکس ، هیمونموتوراکس و empyema (pus ) استفاده میشود درجمع نمودن مایعات موثر میباشد درحمایه تنفس کمک کننده میباشد . • Drainage of fluid or air from pleural cavity • Is used to treat pneumothorax, heamothorax, hemopneumothorax, and empyema (pus) • Is effective to collect fluids. • Is helpful to support breathing
Chest Tube Equipment • Sterile gown, gloves, mask, drapes, and gauze • Chlorhexidine or betadine • 22 or 25 Gauge needle, 10 cc syringe, 1-2% Lidocaine • Scalpel with 11 blade • At least 4 Kelly curved clamps or artery forceps • Strong, non-absorbable sutures size 1.0 or greater (silk or nylon) • Sterile drainage system
Chest Tube Size • Appropriate chest tube size • Chest tubes sized by internal diameter • Length marked on side of tube • Radiopaque strip runs length of tube and encircles the most proximal drainage hole • Choosing appropriate size depends on clinical indication for chest tube • Stable patient with large pneumothorax: 16-22 French • Unstable patient, chronic lung disease, high air leak risk: 24-28 French • Empyema, pneumothorax in patient on ventilator: 28-32 French
Chest Tube Procedure • Obtain and review a chest x-ray prior to procedure • Occlude proximal free end of chest tube with forceps • Occlude insertion end of tube with forceps, this will help with insertion of tube • Place patient in supine position, move ipsilateral arm behind patient’s head
Locate Site of Entry • Triangle of Safety • Lateral border of pectoral major muscle • Mid-axillary line • Horizontal line from the nipple • 4th or 5thintercostal space
Preparation of the Incision Site • Clean region with betadine or chlorhexidine • Apply analgesia • 25G needle form superficial wheel • Inject subcutaneous tissue • Using longer needle inject lidocaine into • Deeper subcutaneous tissue • Numb the periostium of the rib below insertion site
Preparation of Insertion Site • After anesthetizing the periostium advance needle overtop of the rib • Aspirate every 1-2 cm and inject lidocaine • Using scalpel make 2 cm incision parallel but just above the rib
Formation of Tract • Insert Kelly clamp through incision • Use blunt dissection technique and advance over rib • Kelly clamp will “pop” through parietal pleura
Formation of Tract • Use index finger to trace tract created by Kelly clamp • Using forceps direct tube through tract using finger as guide
Advancing Tube • Advance tube toward lung apex in patients with pneumothorax • Advance tube toward base in patients with hemothorax, chylothorax or pleural effusion • Advance tube until you are sure all drainage holes are inside parietal pleura
Securing Chest Tube • Secure tube to skin using heavy suture • Mattress or several simple interrupted sutures to close the hole around the tube • Use the free ends of the suture to wrap around the tube several times • Tie the free ends of the suture around the tube
Preventing Air Leak • Surround the tube with petroleum based sterile gauze • Cover the gauze with several pressure dressings
Confirming Placement • Confirm proper placement of chest tube with chest x-ray. • Using the radio opaque stripe, make sure all drainage holes are contained inside the pleura. • If they are not, replace the tube, DO NOT ADVANCE existing tube
Proper and Improper Chest Tube Placement Improper Placement Proper Placement
Connecting the Chest Tube to Drainage • Connect the chest tube to a sterile draining system • Unclamp the tube • Place drainage system at least 40 inches below the patient
Complications • Bleeding • Traumatic organ injury or perforation • Intercostal neuralgia from damage to intercostals neurovascular bundle • Subcutaneous emphysema • Re-expansion pulmonary edema • Infection of the drainage site • Empyema
Managing Chest Tubes • Pain • Often referred to ipsilateral shoulder • Pain Control • Epidural • Toradal IV
Managing Chest Tubes: Drainage System • Three functional chambers to a drainage system • 1st Chamber: collects fluid/air from patient • Fluid accumulates in 1st Chamber 1
Managing Chest Tubes: Drainage System • 2nd Chamber: Air rises from 1st chamber enters 2nd chamber from below • Water seal will “bubble” • Height of water in 2nd chamber indicates amount of suction 2
Managing Chest Tubes: Drainage System • 3rd Section is an atmospheric vent • Manually venting through a pressure relief valve • It equilibrates collection chamber with atmospheric pressure 3
Managing Chest Tubes: Suction • Amount of suction depends on indication • Spontaneous air leak: start at -10 cm water and use least amount needed to maintain full expansion • Collapsed lung due to PTX: use low gradient to avoid re-expansion pulmonary edema • Fluid Drainage: start at -20 cm of water
Troubleshooting: Air Leak • Continuous bubbling in water seal chamber • Leak is between patient and water seal • Actions: • Tighten loose connections • Locate Leak • If that doesn’t work …
Troubleshooting: Air Leak • Clamp tube near chest wall • If bubbling stops then leak is inside thorax • Get CXR • Call Attending Physician • If bubbling continues then air leak is between clamp and drainage system • Slowly move the clamp from the thorax to the collection system • If bubbling stops at any point in time you have found the leak in the tube • Replace Tube • If bubbling doesn’t stop, leak is in collection system • Replace collection system
Troubleshooting: Tension Pneumothorax • Patient is in respiratory distress even with chest tube in place • First: make sure chest tube is not obstructed • Clamped • Occluded • Kinked
Troubleshooting: Tension Pneumothorax • Drain tubing contents into a separate drainage bottle • Make sure water seal is connected • Make sure water-seal is not broken • If patient has signs of tension PTX, call attending and prepare for a second chest tube placement
Conclusions • Tension Pneumothorax is a life threatening event that can be quickly treated with needle decompression • Chest tubes are used to treat many pulmonary conditions • Proper technique will minimize complications • Careful management of chest tubes will expedite their removal and improve patient status