Download
1 / 31
400 likes | 907 Views
Monitoring CO Poisoning with the Rad-57 TM. Includes a review on Carbon Monoxide Poisoning For Emergency Responders. V.10 14 Dec 11. Important Notice.

E N D
Monitoring CO Poisoningwith the Rad-57TM • Includes a review on Carbon Monoxide Poisoning For Emergency Responders V.10 14 Dec 11
Important Notice • This program is not meant as a substitute for a program or course of study in carbon monoxide recognition and treatment, or emergency medicine. This is for review only. Please refer to your physician or local Medical Director for approved content and medical protocols. • This program is not meant as a substitute for the manufacturer’s operator manual for the Masimo Rad-57. Please refer to the manufacturer for complete operating instructions.
Section 1 Carbon Monoxide Poisoning For Emergency Responders
Introduction • Leading cause of poisoning deaths in industrialized countries: • 50,000 emergency room visits in the US annually 1 • At least 3,800 deaths in the US annually 2 • 1,400-3,000 accidental deaths in the US annually 3,4 • More frequently involved in fatal work-related inhalations than any other substance • 35% of fatal inhalations 5,6 • 1Hampson NB, Weaver LK. Carbon Monoxide poisoning: A new incidence for an old disease. Undersea and Hyperbaric Medicine 2007;34(3):163-168. • 2 Mott JA, Wolfe MI, Alverson CJ, MacDonald SC, Bailey CR, Ball LB, Moorman JE, Somers JH, Mannino DM, Redd SC. National Vehicle Emissions policies and practices and declining US carbon monoxide-related mortality. JAMA 2002;288:988-995 • 3 Hampson NB, Stock AL. Storm-Related Carbon Monoxide Poisoning: Lessons Learned from Recent Epidemics. Undersea Hyperb Med 2006;33(4):257-263 • 4 Cobb N, Etzel RA, Unintentional Carbon monoxide-related deaths in the United States, 1979 through 1988. JAMA 1991;266(5):659. • 5Valent, F et al. Fatal Work-Related Inhalation of Harmful Substances in the United States. Chest. 121:969-975, 2002. • 6Lofgren DJ. Occupational Carbon Monoxide Poisoning in the State of Washington, 1994-1999. Applied Occup and EnviHyg. 17(4):286-295, 2002.
Chemistry • Colorless, Odorless, Tasteless • Chemical Asphyxiant • Vapor Density- 0.97 • Atmosphere- 1.0 • Combines with hemoglobin to form carboxyhemoglobin. • Carbon Monoxide = CO Carbon Dioxide = CO2 • CO = Pulse CO-Oximetry CO2= Capnography
Incomplete combustion of any carbon-based material will produce carbon monoxide. Common sources: Remember, CO is a gas. If it’s found in one area of a building, hotel, apartment, house- assume its everywhere until proven otherwise! Common Sources Lofgren DJ. Occupational Carbon Monoxide Poisoning in the State of Washington, 1994-1999. Applied Occup and EnviHyg. 17(4):286-295, 2002. Erdogan, MS et al. Occupational Carbon Monoxide Poisoning Among West Virginia Workers’ Compensation Claims: Diagnosis, Treatment, Duration, and Utilization. J OccupEnvi Med. 46(6):577-583, 2004.
Pathophysiology Hypoxia- hemoglobin binds CO with a greater affinity than oxygen. Vasodilation- secondary to increased formation of Nitric Oxide Headache, Hypotension, Syncope Intracellular toxicity- Cardiac and skeletal muscle dysfunction Results in short term (acute) and long term (chronic) symptoms. The organs most oxygen dependent are the most affected: the heart and the brain. Hampson NB. UHM 2007. 34(3):163-7.2 Hampson NB et al. Crit Care Med. 2009; 37(6): 1941-47. Bledsoe BE. Journal of Emergency Medical Service. 32:54-59, 2007. Weaver LK, et al. N Engl J Med, 2002;347(14):1057-067. Henry CR, et al. JAMA. 2006;295(4):398-402.
Neurologic Effects Acute Symptoms: CONFUSION Headache Dizziness Seizures Chronic Symptoms: Cognitive/Personality changes Permanent seizure disorders Learning disabilities Early onset Alzheimer’s Disease, Parkinson’s Disease Delayed Neurologic Syndrome Can take up to 8 months before symptoms manifest Hampson NB. UHM 2007. 34(3):163-7.2 Hampson NB et al. Crit Care Med. 2009; 37(6): 1941-47. Bledsoe BE. Journal of Emergency Medical Service. 32:54-59, 2007. Weaver LK, et al. N Engl J Med, 2002;347(14):1057-067. Henry CR, et al. JAMA. 2006;295(4):398-402.
Cardiac Effects Acute Symptoms: Decreased oxygen supply interrupts normal function Decreased oxygen to body Irregular heart beat Chronic Symptoms: Increased risk of early heart disease, heart attack or death. A single exposure to carbon monoxide can result in permanent heart and/or brain damage. Chronic exposure to low levels of carbon monoxide can be worse than a single, large exposure!! • Hampson NB. UHM 2007. 34(3):163-7.2 Hampson NB et al. Crit Care Med. 2009; 37(6): 1941-47. Bledsoe BE. Journal of Emergency Medical Service. 32:54-59, 2007. Weaver LK, et al. N Engl J Med, 2002;347(14):1057-067. Henry CR, et al. JAMA. 2006;295(4):398-402. 5 Weaver LK, et al. N Engl J Med, 2002;347(14):1057-067. • 6 Henry CR, et al. JAMA. 2006;295(4):398-402.
CO Poisoning 30-50 % of CO-exposed patients presenting to Emergency Departments were misdiagnosed. Barker MD, et al. J Pediatr. 1988;1:233-43 Barret L, et al. Clin Toxicol. 1985;23:309-13 Grace TW, et al. JAMA. 1981;246:1698-700
Signs and Symptoms • Carbon monoxide poisoning CANNOT be reliably diagnosed from the patient’s signs and symptoms. • Patients can be sick and not have any complaints. • Symptoms are often vague and mimic other conditions. • Common symptoms include:
Treatment Considerations Protect yourself and your crew: Consider SCBA Remove patient(s) from poisonous environment Treatment for elevated CO is 100% oxygen. With a mask or intubation, per patient condition. Monitor carboxyhemoglobin level with Rad-57. Pregnancy- fetal Hb has a stronger bond to CO than adult Hb A fetus does NOT tolerate hypoxia well Consider transport, even if mother asymptomatic
Half Life Half-life: The amount of time required to reduce the carboxyhemoglobin level by 50%. Age and health will impact the half-life of CO. Breathing Room Air: ~4-6 hours High Flow Oxygen: ~40-60 minutes Placing patients on high flow O2assoonas possible can significantly reduce the damage from carbon monoxide.
Atmospheric CO vs. SpCO Gas monitors measure how much CO is in the atmosphere at that moment in time. It does not tell how much CO is actually inside the patient(s). Doors and windows may be opened prior to arrival, ventilating the house and masking the actual level of CO patients were exposed to. How much is in the air and how much is in the patient are two different things. For example- if the CO level in a patient’s house is 30ppm but has been like that for 4 months, they may be sick. Treatment decisions SHOULD NEVER be based on atmospheric readings alone! Need to factor in: atmospheric readings, SpCO level, patient’s presentation, medical history and the duration of exposure.
Firefighter Risk CO poisoning is often unrecognized due to the presence of exhaustion, heat stress, illness or injuries. CO levels typically highest post-fire, during overhaul. Often SCBA’s not worn during this time. On the fire ground, elevated CO levels can be immediate threats to health and safety: Impaired judgment, confusion Fatigue Exacerbation of pre-existing conditions
Firefighter Rehab • NFPA 1584 suggests monitoring CO levels in FF • CO induces death secondary to V Fib • VF initial rhythm in 90% interior FF deaths • Should not leave rehab if > 5% COHb
Section 2 The RAD 57 Pulse CO-Oximeter™
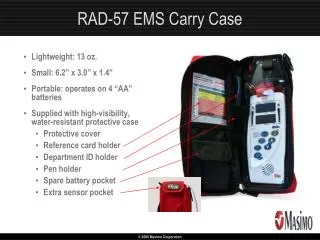
Rad-57 Carry Case Water resistant, protective case Extra sensor pocket Quick Reference Guide pocket Pen holder Spare battery pocket For maximum protection, the device MUST remain in the protective case during field use.
Sensor Placement Step 1: Select the appropriately sized sensor for the patient’s finger Step 2: Carefully insert the patient’s finger into the sensor until it reaches the digit stop. Step 3: Shield the sensor in environments with excessive ambient light 3 STEPS FOR PROPER SENSOR PLACEMENT: Optimal LED path
Sensor Placement Tips Pedi Sensor- Small/slender fingers Adult Sensor- Average to large fingers Sensor should be used on fingers only. Do NOT use toes or ears. Using the non-dominant hand, the following order is preferred: Ring, middle, index finger. Ensure sensor is right side up- the cable should run over the top of the hand. To adjust the sensor or take additional readings,remove the sensor from the finger completely for at least 5 seconds, then replace. INCORRECT SENSOR PLACEMENT MAY CAUSE INACCURATE SpCO READINGS! Adult Sensor Pedi/Slender Digit Sensor
Ambient Light Shield Shield the sensor from intense ambient light! Especially strobe lights or bright sunlight. High-intensity light can interfere with the ability to calculate an SpCO reading. Boot shield Insert the sensor all the way into the light shield; the cable should come out of the top of the opening. Once sensor is in light shield, insert finger into sensor. Bag shield Place sensor on finger first Place bag over sensor and secure with Velcro strap If neither type of shield is available, anything that completely covers the sensor will do- i.e. jacket, pillow, blanket. This does NOT include your hand. Apply pressure to open sensor
Power Up Power Button Press to turn ON Press and HOLD to turn OFF Do NOT have to turn the device on/off in between readings. Battery Life Indicator 4 Green LED’s Each represents ~25% battery life Do Not use rechargeable batteries Battery Compartment Located on the back of device Holds 4 AA alkaline batteries Provides 8-10 hours of battery life
Start Up Sequence Upon power up, the Rad 57 performs a self test Display screen will cycle through alarm setting No external calibration needed. Take ~10 seconds When display shows SEN OFF, device is ready If device fails self test, machine will alarm very loudly. Take out the batteries and call (800) 326-4890. To begin monitoring, apply sensor Calculation/Pulse search: Display will show scrolling zeroes followed by dashed lines. Can take ~20 seconds for SpO2; up to 120 seconds for SpCO.
Measuring SpO2 and Pulse Rate Oxygen saturation (SpO2) reading on top inRED; pulse rate onbottom in GREEN. SIQ- Signal Identification and Quality. Identifies the quality of the SpO2 signal. Press YELLOWbutton to silence alarms for 120 seconds. Press button toscroll through display screens. Next/Enter/Up & Down Arrows- for higher menu functions (i.e. change alarm settings or screen brightness). Alarm Silence Button
Measuring SpCO Press button to switch to the CO screen. Carboxyhemoglobin (SpCO) on top, in %; letters ‘CO’ on bottom May take additional time for the SpCO reading, even if the device already shows the SpO2 and pulse rate. Will see dashed lines on the display while the device calculates the SpCO value. Confirm all elevated SpCO readings by checking sensor placement and repeating the measurement. If SpO2 < 90% or SpMet > 2%, SpCO may NOT display. If SpCO reading is disrupted, display will show dashed lines.
Measuring Perfusion Index (PI) Press the button to cycle to the PI parameter. PI = Measurement of blood flow to the extremity the sensor is on. Similar principal as capillary refill Values range from 0.02-20. The lower the number, the lower the perfusion. Displayed both numerically and graphically. Perfusion Index Bar Graph
Optional Features Auto ON/OFF Device can automatically power down after 5, 10 or 15 minutes of inactivity. Factory Default: Device stays on until the power button is pressed. Perfusion Index (PI) Digital display can be turned on or off PI will always display on bar graph Factory Default: PI display is on. Start up screen Upon powering on, can select SpCO screen to display first. Factory Default: SpO2/pulse rate parameters will display first.
SpCO Accuracy The accuracy of the SpCO parameter is +/- 3% for 1 standard deviation within a range of 1 to 40%. Said another way, the RAD 57 will be within 3% of a blood gas 68% of the time and within 6% of a blood gas 95% of the time. Example: If a patient has a SpCO of 5%, their carboxyhemoglobin could be as low as 2% or as high as 8%. Measurements may vary from reading to reading, even on the same patient, within the accuracy specification. If 2 readings vary greatly (i.e.- one finger reads 3%, another finger reads 10%): Confirm the proper sensor is being used Confirm proper sensor placement technique Shield the sensor from light Repeat readings
Obtaining Accurate SpCO Measurements Inaccurate SpCO measurements may be caused by: Incorrect sensor placement Excessive ambient light Low arterial perfusion Patient motion Altitude-induced hypoxemia Low arterial oxygen saturation Elevated levels of methemoglobin Intravascular dyes or externally applied coloring (such as nail polish)
Thank You QUESTIONS?