Download
1 / 62
740 likes | 1.47k Views
Essentials of Oral Pathology Volume I. Introduction to Oral pathology. Is the study of diseases affecting the oral cavity. ِ A new designation for this ; is oral & maxillofacial pathology. Early recognition & microscopic examination are the ways to determine the true nature of the disease.

E N D
Essentials of Oral Pathology • Volume I
Introduction to Oral pathology • Is the study of diseases affecting the oral cavity. • ِ A new designation for this ; is oral & maxillofacial pathology. • Early recognition & microscopic examination are the ways to determine the true nature of the disease. • The dentists must be able to recognize abnormalities of the oral cavity & surrounding tissues. • Upon recognize an abnormality , the dentist is also expected to create a list of disease , it may present as differential diagnosis. • He also expects to take a biopsy & send the tissue sample to a qualified pathologist. • It is often impossible to determine the nature of abnormalities by their clinical appearance.
Classification of Oral diseases : Traditional classifications group oral diseases : • by microscopic appearances ( fibro-osseous lesions) , • by their presumed origin ( Odontogenic & non odontogenic ) or • by their location ( bone diseases)
Some clinical features of oral lesions: 1) The colour of the lesions : -Oral lesions may be red , white , yellow , brown or black. - These colours are caused by changes in cells & intercellular materials of which lesions are composed by observing the colour showed by lesion & think about the tissue changes that may have produced it , the range of possible diseases will be considerably narrowed. Red lesions may be due to : - dilated blood vessels - inflex of new blood vessels - thin overlying epithelium or - hemorrhage under the surface.
White lesions may be due : - increased surface keratinization - increased thickness of epithelium ( acanthosis) - death of the surface epithelium or - development of surface fungal colonies. • Blue lesions are due to dilated blood veins • Yellow lesions are due to fat deposits. - Brown lesions are due to melanin pigmentation in mucous - Implanted amalgam or extruded melanin pigmentation may produce black lesion
2- Surface lesion of the mucous membrane elevated - Macule is a flat discolored spot not raised above the surface - Plaque is defined as any discolored patch or flat area - Ulcers & erosions are depressed lesions. - If the defect is a deep one exposing the lamina propria , the term ulcer is used to describe it. Shallower defects that do not expose the underlying tissue are often called erosions. - Papules , papillae , polyps & verruca are elevated surface lesions.
- If the elevation is thicker & nipple like the term papilla is used. - An elevation of softer consistency is a polyp. A warty lesion having many small papillae extending from it is verrucous growth. - Lesions situated under the mucosa produce lumps & called submucosal lesions, do not alter the surface colour or texture . - The only evidence of disease is a bump نتوء أو ورم that may be seen by touch or sight .Small submucosal bumps are known as nodules while larger ones are known simply as masses . 3- Lesions within the jaws : - Are detected as radioluecencies, radioopacities or mixed radiolucent opacities on radio graphic examinations. -There are a number of oral diseases that arise within mandible or maxilla . - If the disease replaces bone with uncalcified “ soft tissue” the resulting lesion will appear as a dark spot or radiolucency.
- If the lesion is a slow-growing one , surrounding bone will have time to create a dense layer demarcating it. In these cases the radiolucency will be surrounded by a radio opaque border. - On the other hand , if the lesion is faster growing , it will not demarcated by radioopaque line. - Radioopacities are caused by diseases that produce calcified materials that impede the passage of x –rays. - If a disease produce both soft & calcified tissue a mixed radiolucency radioopacities will result, appear as mattled خليط dark & light radiographic areas, A group of conditions in which acute & chronic inflammations occur ,These conditions may accompanied by pain ,swelling & pus formation. * On the other hand , there are other diseases caused by bacterial fungal or viral infections could occur in the oral cavity as oral manifestations of these systemic disease.
These lesions are of great interest to the dentists because the early diagnosis of these conditions could be made in the dental clinic. • Moreover , these conditions are often contagious , so self protection by dentists could be achieved.
contents • Chapter 1Developmental disturbances of teeth • Chapter 2 Dental caries • Chapter 3 Pulp & periapical lesions • Chapter 4 Odontogenic cysts & other cysts of the jaws & para - oral region. • Chapter 5 Odontogenic tumours.
Developmental disturbances of teeth & calcified dental tissues - Normal tooth development : normal teeth development are divided into two different stages which are : - Morphologic stages : 1- Dental lamina 2- Bud stage. 3- Bell stage ( early & late) - Histophysiologic stages : 1- Initiation number 2- Proliferation size + shape 3- Histodifferentiation structure 4- Morphodifferentiation shape 5- Apposition structure
Development of an ideal dentition depends on many factors : 1- Normal formation of a completed number of dentition 2- Normal shape & size of the teeth. 3- Normal structural development of the dental tissues. 4- Normal date of eruption of both dentitions. 5- Correct relationship with opposing . Abnormal tooth development will be as a result of many factors such as hereditary , racial , systemic or local. Disorders of development of the teeth will be one or more of the following : 1- Variations in number 2- Abnormalities in the size. 3- Anomalies of the shape. 4- Structural defects 5- Disorders of eruption.
I. Variation in number : 1- It occurs during the initiation stage of the tooth development , mostly the permenant ones. 2- Variation in number of teeth may be either , the condition of decrease or increase of number of normal dentition. 3- 1-3% of population have either extra teeth or missing permanent teeth Decrease in number Anodontia: Absence of single or group or complete absence of teeth. It is due to failure of tooth development during initiation stage. Types of anodontia : Total anodontia 1) A total absence of all teeth of one or both dentition ( more common permenant). 2) A complete failure of tooth development . 3) It may be : 1. associated with other ectodermal defects ( e.g. hereditary ectodermal dysplasia ). 2. Unassociated with other ectodermal abnormalities.
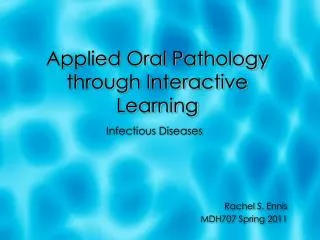
Total anodontia Partial anodontia
oligodontia congenitally missing bicuspid microdontia or "peg lateral" ectodermal dysplasia
Hereditary ectodermal dysplasia = Streeter,s syndrome: - A hereditary condition in which the patient is suffering from deficiency in ectodermal structures such as ( skin , nails , glands , brain & hair) Etiology: 1) Hereditary it is transmitted as a sex-linked recessive character . 2) It is transmitted through females & affect mainly the males Moreover married relative leads to increase the incidence . Clinical picture : 1) Skin : thin , dry , shiny & smooth. 2) Hair : absent or scanty , dry unhealthy ( especially scalp , eye , lashes & eye brows ). 3) Brain : sometimes mental retardation occurs 4) Anemia 5) Glands :
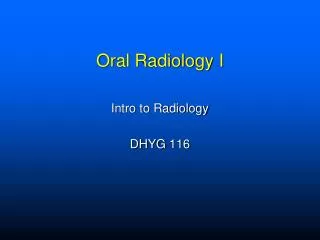
Typical cleft lip/palate and maxillary hyperplasia in a patient with Rapp-Hodgkin syndrome. Hands of father and son with Rapp-Hodgkin syndrome. Nails have the same characteristics; they are brittle, thin, and dystrophic. Wrinkled, hyperpigmented skin around the eyes and everted lips are typical characteristics of anhidrotic/hypohidrotic ectodermal dysplasia syndrome A newborn boy with anhidrotic / hypohidrotic ectodermal dysplasia syndrome showing generalized fine scaling and a history of intermittent fever. Ectodermal dysplasia, ectrodactyly, and clefting syndrome. Light-colored hair and scalp and earlobe defects are observed. Cleft lip and palate results in a characteristic nasal contour. Ectrodactyly observed in an individual with ectodermal dysplasia, ectrodactyly, and clefting syndrome.
A- sweat gland : they are absent –deficient sweating , thus no perspiration .First symptom is intolerance to hot weather ( Anhidrosis) B- Sebaceous gland : Absent – No sebum , so dry skin. C- Salivary gland : Absent – ( salivary gland which lead to dry mouth xerostomia D- Mucous gland : - in nose : dryness , leading to rhinitis .- in pharynx : dryness , leading to pharyngitis & dysphagia 6- Normal growth of jaw 7- Total anodontia
II) Partial anodontia affecting group of teeth : 1-True : - A very rare condition as a part of Streeter,s syndrome . - Teeth were not developed. -This is confirmed by x ray. -It has a hereditary base 2- Pseudo : 1)The teeth were developed but failed to erupt either due to : Impaction: No sufficient space for eruption Imbeding : No force of eruption 2) Teeth are present in x ray 3) multiple impacted supernumery teeth are present in cleidocranial dysplasia 3- False : The teeth are not present in x ray or in the oral cavity due to - extraction - or trauma
Increase in number of teeth: Extra teeth = additional teeth : This condition may be supplemental or supernumary teeth. Supplemental teeth ( resemble normal teeth) The most common sites are : upper lateral , lower second premolar & third molar. 1) Upper lateral incisor : 22 22 It is due to : 1) complete division of enamel organ of normal upper lateral OR 2) Extra tooth germ from dental lamina 2) lower second premolar : 55 55 It is due to extra tooth germ from dental lamina 3) Third molar 88 88 - It is due to extra tooth germ from dentinal lamina - It may be due impacted & later on erupted after extraction of teeth & using denture In this condition it is called fourth molar . 4) Post permanent dentition & it is due to deep growth of dental lamina after giving normal dentition 5) Predeciduous dentition It is a congenital condition characterized by presence of teeth in mandibular incisor region in newly born infant . It is due to extra tooth germ before giving origin to tooth germ of deciduous teeth .
Anhidrotic ectodermal dysplasia showing conical teeth, giving an undesirable, Dracula-like appearance.
By X ray : the deciduous teeth are present in the jaw. Supernumeray teeth ( not resemble normal teeth ) : - They are classified according to their site in dental arch into : 1) Mesiodens : Site : In the mid – line between the upper central incisors . Shape : conical or peg-shaped . It may be as : - A single or doubled - Erupted or impacted -Inverted or Erupt in the floor of nose when inverted. Clinical significans : May cause : 1) separation of two central incisors. 2) prevention of eruption of one of centrals. Mesiodens occurs most commonly in males more than males 2) Paramolar : shape : cone shaped Site : more common at buccal aspect of upper & lower molar . It may be as : 1- A separate denticle ( cone shaped independent ) , or 2- Fused to neighbouring molar . 3- As an extra cusp of the related molar.
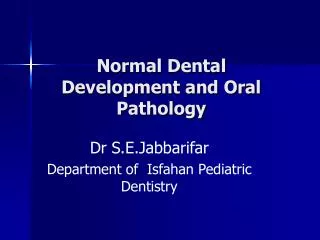
Slide 1: mesiodens Slide 2: fourth molar Slide 3: supernumerary bicuspid Supernumerary Teeth Slide #1 is an example of an extra incisor. When located in the midline between the two permanent central incisors, they are referred to as mesiodens. Slide #2 depicts an extra molar tooth (a paramolar) and Slide #3 is an example of a supernumerary bicuspid tooth. These are the most common supernumerary teeth in the order shown.
3) Distomolar : Shape : peg – shaped Site : Distal to upper third molar It may be as : 1) A separate denticle peg أسفين shaped , or 2) Fused ( extra distal cusp) . Cleidocranial Dysplasia ( Dystosis) : - It is a rare hereditary disorder characterized by deficiency in membranous & cartilagenous bone formation . - It is a hereditary condition transmitted by an autosomal dominant gene. Clinical picture : Age : Infants. Sex : both sexes. Site : membranous & catilagenous bones such as clavicle , cranium , mandible & maxilla . .
Cementum analysis Dystosis
Characters : 1) Clavicle : -Unilateral or bilateral Absence - Complete or partial The patient can approximate his shoulders at the midline 2) Cranium : - Delayed closure of fontalls. - Prominent frontal bone. - Under developed paranasal sinuses. - Depressed nasal bride. 3) Maxilla : - Underdeveloped . - V-shaped . - High arched palate . - Cleft palate 4) Mandible : - Unaffected . - Relative prognathism بروز الفكين
5) Dental anomalies in cleidocranial dysplasia : 1) Deciduous erupt normal but failure of shedding. 2) Late eruption in permenant dentition. 3) By X ray multiple impacted supplemental & supernumeray teeth. 4) Dentigerous cyst. 5) Enamel hypoplasia 6) Hooked roots. 7) Conical teeth. 8) Germination 9) Absence of cellular cementum Variation in the size : Due to abnormal proliferation stage of tooth development : 1) Increase proliferation 2) Decrease proliferation
8 • Bilateral generally • Hormonal gigantism
8 Variation in the shape : Abnormal proliferation & morphodifferentiation Double or connated & teeth ( born together)
3) Dilaceration تخريب Definition: - It is a sharp bend or curve occurs in the crown , between crown & root or along the root during tooth development. - It may be due to : - Trauma applied to deciduous tooth will push it into the socket where it affect the developing tooth germ of permanent tooth. Pathogenesis : - After mild trauma the already calcified part will move along the direction of trauma while the uncalcified part of the tooth being soft & reslient will not suffer any change in it is position. - Usually dilaceration occurs in the anterior permanent teeth. Clinical significance : 1- Difficulty in extraction . 2- Difficulty in root canal filling .
Enamel-Dentine Fractures (Type II) Enamal Fractures (Type I) Fractures Involving Pulpal Exposure (Type III) Complete Loss of Tooth (Type V) Crown-Root Fracture (Type IV)
4) Congenital syphilis : 1- It is a developmental condition. 2-The fetus acquired the infection by trapenoma pallidum microorganism from his mother after 4th month of intrauterine life. 3- So , the teeth which are developed during this period of life will undergo malformations ( incisors , canines & 1th molar ). 4- Deciduous teeth are not affected because they are developed before the 4th month of intrauterine life. 5- The perivascular edema will cause bilging of the ameloblastic layer into dentine papilla . 6- So the permenant teeth which are commonly affected : - Upper central incisor -1th molars Dental stigmata of congenital syphilis : 1- Hutchinson,s tooth. 2- Moon, s molar. 3- Mulberry molar. 1) Hutchinson,s incisors: 1- The tooth affected is upper permanent central incisors. 2- The tooth is barrel – shaped. 3- The mesial & distal surfaces are converging in the incisal half. 4- The mesial & distal angles are rounded. 5- The incisal edge have notch ( screw driver appearance). 6- The enamel surface show enamel hypoplasia Notched incisors known as Hutchinson's teeth which are characteristic of congenital syphilis
2) Moon,s molar : 1- The affected tooth is 1st molar . 2- The occlusal surface is ( Dome-shaped). 3- The surface show enamel hypoplasia 3) Mulberry molar : 1- The affected tooth is 1st molar. 2- The occlusal surface show multiple cuspules replicating the normal – cuspal pattern ( so the surface is rough & pitted ) 3- The surface show enamel hypoplasia . N.B. : Hutchinson,s triad of congenital syphilis : 1- Hutchinson,s incisor 2- Deafness 3- Interstitial keratitis .
A photograph of Moon’s Molar or Mulberry Molar resulting from congenital syphilis. Description Moon's- or Mulberry Molar is a condition where the first lower molar tooth has become dome-shaped due to malformation by congenital syphilis.
5) Taurodontism : ( bull-like teeth) - In which the crown of the tooth is enlarged on the expense of the roots Classification: A) Hypotaurodontism ( the mildest form ) B) Mesotaurodontism C) Hypertaurodontism - There is no constricted neck & bifurcation is near to the apices of roots. - It is due to failure of epithelial root sheath of Hertwig,s to invaginate at the proper – horizontal level of forming root. Clinically:- affects mostly molars. - It may be unilateral or bilateral Discovered by X ray : * A huge pulp chamber & * No constricted neck & * Small short roots with short area of bifurcation . * Easy extraction of taurodont
gemination fusion concrescence dilaceration Germination of both central incisors
6) Invaginated odontome : - Other name : Dens invaginatus - It is due to invagination of the enamel organ into dentin papilla during tooth development. Site : At the cingulum area ( accentuated palatal pit) Affected tooth : Maxillary central & lateral incisors Radiographs reveals an invagination lined enamel which is continuous with the normal enamel covering of the tooth. - This resembles a tooth within a tooth ( Dens in dente) Clinical significance : - Collection of food debris. - Development of dental caries.
7) Evaginated odontome : Other name = Dens evaginatus It is due to evagination of a part of enamel organ & subsequent evagination of dentine papilla . Site : Occlusal surface Affected tooth : Premolars. Race : Caucasian & mongol Clinical significance : - Fracture of this extra cusp . - Development of dental caries. 8) Enamel pear ( enameloma) * Droplet of enamel on the root of the tooth Site Near the furcation of the roots of maxillary permanent molar or close to cemento enamel junctions or at root apex. Pathogenesis : Disturbance of growth of epithelium . Root sheath of Hertwig,s resulting in budding of the sheath lead to differentiation of ameloblasts & amelogenesis.
Enamel pear -A small, spherically shaped enamel projection on a root surface is called an enamel pearl. It is usually seen on maxillary molars in the furcation area. This photograph shows the mesial view of a maxillary third molar.
Abnormalities of structure of teeth These structures defects occur during histodifferentiation & appositional stages of tooth developemnt
Hereditary structure defects of enamel ( amelogenesis Imperfecta ) : A hereditary defect of enamel formation which is transmitted through more than one mode of genetic transmission . Two forms of amelogenesis imperfecta are seen : I) Hereditary enamel hypoplasia . It is one form of amelogenesis imperfecta in which the defect is quantitative reflected in a decrease in the AMOUNT of organic matrix Histopathology : ( in long.ground sec.) 1- Small area of enamel show the normal prismatic structure . 2- The rest of the enamel shows hyaline glossy appearance with fine laminations parallel to tooth surface. II) hereditary enamel hypocalcification: It is a form of amelogenesis in which the defect in mainly qualitative reflected in defecient MATURATION & MINERALIZATION . Clinical picture : - Enamel is soft to the probe. - Lack of surface luster ( opaque matt surface). - Enamel wears easily so exposing dentin which wears also down rapidly may get to gum line.
Histopathology : 1- Prismatic structure is maintained 2- Surface layer of lamination is present
Acquired enamel hypoplasia : - Acquired enamel defects are usually confined to permanent dentition ( except in cases of dental fluorosis) I) Acquired enamel defects due to local factors : 1) Trauma : - Trauma to upper deciduous incisors may push them deeply into their sockets resulting in their roots impiging يصطدم upon the developing tooth germs of the permanent successors. - This may lead to horizontally oriented hypoplasia running between the previously calcified enamel & that which is yet not calcified. 2) Infection : ( Turner,s tooth ) - Periapical infection of deciduous tooth especially the molars may reach the underlying developing tooth germs of premolars. -This may lead to horizontally oriented hypoplastic defects in enamel surface , which is seen either thin , irregular or even completely absent over certain areas of the tooth. - Severe infections ( e.g. osteomyelitis ) may also affect the structure of enamel & dentine or may even completely arrest the development ( stunted tooth ) 3) Radiotherapy
II) Acquired enamel defects due to systemic factors : May systemic factors may cause toxic damage of ameloblasts : 1- Nutritional deficiency ( vit A , D , C ) & minerals ( calcium & phosphorus) 2- Exanthomatous fevers ( scarlet fever , measles & chicken pox ) . 3- Infantile GIT disturbances. 4- Congenital syphilis. 5- Ingestion of chemicals ( fluoride & tetracycline). 6- Birth injury & premature birth. 7- Rh incompatibilty. 8- May be associated with general genetic or idiopathic disorders : A- Cleido – cranial dysplasia . B- Monogolism ( Trisomy 21)