Download
1 / 44
440 likes | 480 Views
Explore the fascinating world of pituitary hormone regulation, function, and associated disorders in this detailed guide. Learn about the history, cell populations, hormonal production, and pathologies of the pituitary gland. Discover the intricate neuroimmunoendocrine regulation and the different pituitary syndromes, including hypofunctional and hyperfunctional conditions. Dive into the complexities of pituitary adenomas and their classification based on endocrine activity, imaging, histology, and more.

E N D
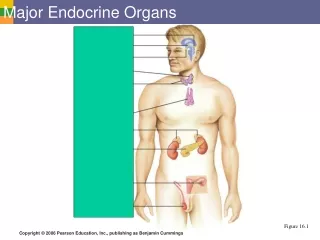
Pathology of the Endocrine Organs - I Pituitary Adrenals Jaroslava Dušková Inst. Pathol. 1st Med. Fac. Charles Univ. Prague https://www1.lf1.cuni.cz/~jdusk/
Pituitary - history - I Galenos (2nd cent.) lat. pituita = gr. phlegm = moisture, mucus A. Vesalius(16th cent.) glandula pituitam cerebri excepiens R. Lower(17.stol.) Dissertatio de origine catarrhi – incretion
Pituitary - history - II Rathke, H.: (1838) Über die Entstehung der glandula pituitaria (Arch Anat. Physiol. u. Wiss. Med. , 5, 482-5) W. Haberfeld(1909) Die Rachendachhypophyse, andere Hypophysengangreste und deren Bedeutung für die Pathologie Beiträge zur path. Anat. u. allg. Pathol. , 46, 133-232)
1. formation of the Rathke´s pouch & proc. infundibularis 2. splitting of the Rathke´s pouch 3. mature formation
Neuroimunoendocrine regulation CRF IL-1 neuronal connections ACTH TNF IL-6 IL-1 n.vagus Glucocorticoids Adrenals Immune cells
Pituitary - regulation Higher neural centra limbic system reticular system hypothalamus liberins & statins adenohypophysis trophic hormons of the adenohypophysis periferal endocrine glands hormons of periph. glands tissues
Neuroimmunoendocrine Regulation Messengers • Neurotransmitters • Interleukins • Hormons
Pituitary – weight Females 505 - 1002 mg (average 660 mg) pregnant women 560 - 1220 mg (average 762 mg) Males 400 - 855 mg (average 570 mg) Rasmussen, AT Am.J. Anat. 1928 a 1934
Pituitary- architecture • adenohypophysis • pars infundibularis (tuberalis) • pars intermedia • neurohypophysis • hypophysis pharyngea (+ hidden islets of pit. cells in the os sphenoides)
Pituitary- cell inclusions • squamous epithelium • Rathke´s pouch between AH and NH • salivary glands- NH, often with oncocytes
Pituitary- parts - function • Adenohypophysis secretion of tropins • Pars infundibularis (tuberalis) modulation of AH secretion • Pars intermedia • Neurohypophysissecretion of neuropeptides • hypophysis pharyngea evtl. secretion of tropins
Pituitary– cell populations • acidophil(somatotrophs, lactotrophs) • basophil(corticotrophs, gonadotrophs, thyreotrophs) • chromofobe(transitional. + foliculostellate) • oncocytes(or preoncocytes) • mesenchymal • pituicytes (macroglie) • secretion neurons(tractus supraoptico- et tuberohypophyseus)
Hypophysis- cell population & hormonal production • acidophil PRL , STH • basophil ACTH, FSH, LH, TSH • chromophobe 0, PRL , STH , ACTH, FSH, LH, TSH • oncocytes 0, PRL , STH , ACTH, FSH, LH, TSH • mesenchymal • pituicytes • secretion neurons oxytocin, vasopresin
Pituitary- cell population & hormonal production Hormonal production mostly mixed (e.g. ACTH+FSH,LH,TSH,PRL)
Pituitary - cell population &hormonal production Individual producents able of interconversion due to stimulation (e.g. PRL-GH)
L e p t i n • adipocytes - blood - CSF -hypothalamus (ncl. arcuatus ) • regulation of energetic homeostasis • correlation with the body fat content • in most obese individuals high levels -resistence? Friedman et al., Nature 1994
Pituitary- regressive changes • Dystrophy(Crooke´s hyaline change) • Atrophy - in aging increased fibrosis, no functional influence • NECROSIS • traumatic (mostly due to the stalk lesion) • ischemic
Pituitary- vascularisation • a. hypophysea sup. (from ACI) • a. trabecularis directly to AH • long portal veins in the stalk • a. hypophysea inf. (from ACI in sinus c.) • short portal veins
incidence 1- 8 % large autopt. series pathogenesis intracranial hypertension ischemia vasospasmus atherosclerosis thrombi stalk lesion healingscar focal regenerates possible meaning hypofunction only in case of more than 3/4 of volume destruction Pituitary- necrosis
non specific (peri)hypophysitis purulenta non purulenta septic pyemic microabscesses lymphocytic autoimmune specific tbc hematogenous dissemination solitary tuberculoma lues inborn acquired Pituitary- inflammation
Pituitary syndromes • Hypofunctional • panhypopituitarismus • selective hypofunction • Hyperfunctional • monohormonal • combined
Total >90% AH destroyed Syndromes: Simmonds Sheehan Falta Lorain Partial monohormonal combined Regulatory hypofunction peripheral glands ectopic production iatrogenous Hypopituitarismus
m. Adisoni centralis • adrenal atrophy • vacuolisation of cardiomyocytes • lack of the skin hyperpigmentation • hypotension • weekness • hyperkalaemia
Pituitary Adenomas 9% • chiasma opticum compression 43 • acromegaly 23 • galactorea-amenorea 7 • hypopituitarismus 7 - most frequent clin. symptomes 9% 54% 28%
The WHO Classificationof Adenohypophysial Neoplasms . A proposed five-tier scheme 1. endocrine activity 2. imaging/ surgery 3. histology 4. immunohistochemistry 5. ultrastructure Kovacs, K., Scheithauer, B., Horvath Eva, Lloyd, R Cancer 1996, 78,502-10
Pituitary Adenomas • acidophillic • basophillic • chromophobe • mixed
Acidophillic adenomas • somatotroph • lactotroph • mixed somatotroph and lactotroph • somatolactotroph densely granulated • onkocytic
Basophillic adenomas • corticotrophic • thyreotrophic • gonadotrophic densely granulated
Chromophobe adenomas • all types of hormonal productions scarcely granulated • null cell
Monohormonal Syndromes: 1. gigantismus/acromegaly 2. hyperprolactinemia (galaktorea, amenorea) 3. Cushing 4. hyperthyreosis 5. (hypergonadotropinismus) Combined 1+2, 1+3, 1+4, 2+3, 3+4 Regulatory hyperfunction periph. glands ectopic production iatrogenous Hyperpituitarismus
Plurihormonal and PlurifunctionalPituitary Adenoma with Acromegaly Syndroma doc. MUDr Jaroslava Dušková, CSc*, prof. MUDr Josef Marek, DrSc**, prof. MUDr Ctibor Povýšil,DrSc*
F 75 yrs • 30 yrs lasting acromegaly • refused surgery • Symptomatic therapy • hyperfunction thyr . – Carbimazol • cardiomegaly - cardiotonica • 5 yrs prior tu death ca coli – surg. removed • 6 yrs prior tu death corticoid substitution • death cardial failure
STH +++ Prl ++ ACTH ++ TSH +++ FSH (beta)+ LH (beta)+ Plurihormonal and PlurifunctionalPituitary Adenoma with Acromegaly
Pituitary INCIDENTALOMA- algorithm of Investigation and treatment
Other Pituitary Tumours • craniopharyngeoma • metastases
Adrenals • cortex • definitive • fetal (90% regression by 6 months of age) • neonate 8g (3,5kg) 0,002 • healthy adult 9g (70kg) 0,0001 • zones G,F,R 20x • medulla
Adrenals - syndromes • hypofunction - panhypocorticalism • acute • chronic – Adison • peripheral • central • hyperfunction • AGS • Cushing • hyperaldosteronismus Conn,Bartter
norm hypoplasia congenitalis
Adrenals - syndromes • hypofunction - panhypocorticalism • acute • chronic – Adison • peripheral • central • hyperfunction • AGS • Cushing • hyperaldosteronismus Conn,Bartter
Adrenals - syndromes • hypofunction - panhypocorticalismus • acute • chronic – Adison • periferic • central • hyperfunction • AGS • Cushing • hyperaldosteronismus Conn,Bartter