Download
1 / 35
420 likes | 1.43k Views
Drugs act on ANS cholinergic agonists and antagonists. Dr. Hashem Mansour. OVERVIEW. Drugs affecting the autonomic nervous system (ANS) are divided into two groups according to the type of neuron involved in their mechanism of action.

E N D
Drugs act on ANS cholinergic agonists and antagonists Dr. Hashem Mansour
OVERVIEW • Drugs affecting the autonomic nervous system (ANS) are divided into two groups according to the type of neuron involved in their mechanism of action. • The cholinergic drugs, which are activated by acetylcholine (ACh). • The adrenergic drugs act stimulated by norepinephrine or epinephrine.
Neurotransmission at cholinergic neurons • Neurotransmission in cholinergic neurons involves six sequential steps: • 1) synthesis • 2) storage • 3) release • 4) binding of ACh to a receptor • 5) degradation of the neurotransmitter in the synaptic cleft • 6) recycling of choline and acetate.
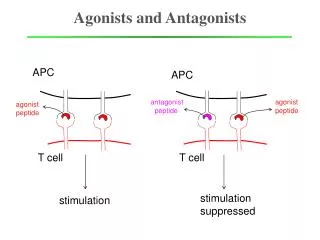
CHOLINERGIC RECEPTORS • Two families of cholinoceptors, designated muscarinic and nicotinic receptors. • Distinguished from each other on the basis of their different affinities for agents that mimic the action of ACh (cholinomimetic agents).
Muscarinic • These receptors are selectively stimulated by muscarine and selectively blocked by atropine. • They are located primarily in heart, blood vessels, eye, smooth muscles and glands of gastrointestinal, respiratory and urinary tracts, sweat glands, and in the CNS.
Subtypes of muscarinic receptor • The muscarinic divided into 5 subtypes M1, M2, M3, M4 and M5. • M1: located in cortex, hippocampus and corpus striatum. • It plays a major role in mediating gastric secretion and relaxation of lower esophageal sphincter caused by vagal stimulation. • M2: Cardiac muscarinic receptors mediate vagal bradycardia. • M3: Visceral smooth muscle contraction and glandular secretions and vasodilatation.
Nicotinic • These receptors are selectively activated by nicotine and blocked by tubocurarine it is two subtypes NM and NN are recognized. • NM: These are present at skeletal muscle endplate They mediate skeletal muscle contraction. • NN: These are present on ganglionic cells, adrenal medullary cells, in spinal cord and certain areas of brain.
CHOLINERGIC DRUGS(Cholinomimetic, Parasympathomimetic) • These are drugs which produce actions similar to that of ACh, either by directly or indirectly. • CHOLINERGIC AGONISTS (direct acting) • Choline esters Alkaloids • Acetylcholine Muscarine • MethacholinePilocarpine • CarbacholArecoline • Bethanechol
ACTIONS of ACh • 1. Heart: Negative ionotropic and chronotropic effects • 2. Blood vessels: All blood vessels are dilated, thus, fall in BP and flushing. • 3. Smooth muscle: Tone and peristalsis in the gastrointestinal tract is increased and sphincters relax → abdominal cramps and evacuation of bowel. • Peristalsis in ureter is increased, the detrusor muscle contracts while the sphincter relaxes → voiding of bladder. • Bronchial muscles constrict → dyspnoea.
ACTIONS of ACh • 4. Glands Secretion from all parasympathetically innervated glands is increased—sweating, salivation, lacrimation. • 5. Eye Contraction of circular muscle of iris → miosis. • Contraction of ciliary muscle → reduction in intraocular tension.
CHOLINOMIMETIC ( direct acting) • Pilocarpine: exhibits muscarinic activity and used primarily in ophthalmology. • 1. Actions: similar to ACh. • 2. Therapeutic use: itis the drug of choice for both open -angle and angle-closure glaucoma. • Treatment xerostomia and Sjogren syndrome
Pilocarpine • Adverse effects: blurred vision, night blindness, and brow ache. • Poisoning characterized by exaggeration of various parasympathetic effects. • Parenteral atropine, is administered to counteract the toxicity of pilocarpine.
INDIRECT-ACTING CHOLINERGIC AGONISTS:ANTICHOLINESTERASE AGENTS • Inhibitors of AChE thus indirectly provide a cholinergic action by preventing the degradation of ACh. • This results in an accumulation of ACh in the synaptic Space. • Therefore, these drugs can provoke a response similar to Ach.
ANTICHOLINESTERASES (ACHEI) • Anticholinesterases (anti-ChEs) are agents which inhibit AChE. • Reversible • Carbamates • Physostigmine • Neostigmine • Pyridostigmine • Irreversible • Dyflos, Echothiophate , Malathion*
ACHEI (organophosphates) • 1.Physostigmine stimulates the muscarinic and nicotinic receptors. • 2. Therapeutic uses: Treatment of intestinal and bladder motility atony. • Treatment of overdoses of a atropine. • 3. Adverse effects: CNS may lead to convulsions at high doses. • Paralysis of skeletal muscle.
TOXICOLOGY OF ANTICHOLINESTERASE AGENTS • Irreversible AChE inhibitors are commonly used as agricultural insecticides • Toxicity with these agents is manifested as nicotinic and muscarinic signs and symptoms (cholinergic crisis).
Treatment of ACHEI toxicity • Pralidoxime: (2-PAM) can reactivate inhibited AChE. • Athigher doses, may cause side effects similar to other AChE inhibitors. • B. Other treatments • Atropine to prevent muscarinic side effects of these agents. • Diazepamis also administered to reduce the persistent convulsion caused by these agents.
ANTICHOLINERGIC DRUGS (Muscarinic receptor antagonists, Parasympatholytic) • Anticholinergic drugs are those which block actions of ACh on ANS and in the CNS.
ANTICHOLINERGIC DRUGS • Atropine, scoplamine, Hyoscine butyl bromide, Ipratropium bromide, Tiotropium bromide, Trihexyphenidyl.
PHARMACOLOGICALACTIONS(Atropine) • 1. CNS Atropine has an overall CNS stimulant action. • Atropine stimulates many medullary centres—vagal, respiratory, vasomotor. • It suppresses tremor and rigidity of parkinsonism.
Atropineffcts • CVS: Heart tachycardia. • Eye: mydriasis, results in photophobia. • Smooth muscles All visceral smooth muscles are relaxed. constipation may occure. • Atropine causes broncho-dilatation • Glands Atropine markedly decreases sweat, salivary, tracheobronchial and lacrimal secretion. • Body temperature Rise in body temperature occurs at higher doses. Children are highly susceptible to atropine fever.
Therapeutic uses of anticholinergic agents • Ophthalmic: Topical atropine exerts both mydriatic • Cardiovascular: Treat bradycardia of varying etiologies. • Antisecretory: Sometimes used in the upper and lower respiratory tracts prior to surgery. • Antidote for cholinergic agonists: Treatment of organophosphate poisoning,
Therapeutic uses of anticholinergic agents • Parkinsonism: trihexiphenidyl hydrochloride. • Motion sickness: Hyoscine is highly effective. • Asthma: Ipratropium bromide.
REHABILITATION FOCUS • Cholinomimetics may enhance or inhibit rehabilitation program. • Scheduling treatment Program will enhance functional or cognitive activities. • In patients with spastic bladder and incontinence, the therapist may reduce inadvertent voiding by scheduling treatment periods.
CLINICAL RELEVANCE FOR REHABILITATION • Adverse Drug Reactions • Shortness of breath and altered heart rate may both occur with muscarinic agonists. • Nicotine may increase blood pressure and possibly resulting cardiac arrhythmias. • Muscarinic agonists can decrease visual acuity by preventing pupillary dilation in response to decreased light. • Antimuscarinics can cause sedation and decrease cognitive function.
Effects Interfering with Rehabilitation • Bronchoconstriction may decrease patients' ability to participate in aerobic activities. • Hyperthermia, increased blood pressure and heart rate can also decrease patient participation in aerobic activities . • Sedation and decreased cognitive function can decrease patients' understanding of instructions for home treatment programs. • Changes in light levels in the room in conjunction with sedation may increase the chance of falls.
Possible Therapy Solutions • To avoid dyspnea and cardiac dysfunction, aerobic treatment prescriptions should be designed to allow the patient more time to achieve their aerobic goal. • If sedation or decreased cognitive function is a problem, consider therapy at the end of a dosage period when the drug's plasma levels will be at their lowest.