Download
1 / 27
280 likes | 423 Views
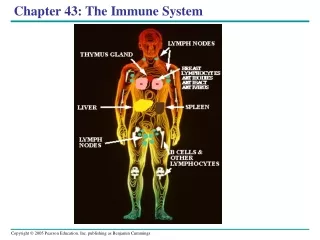
Chapter 5 The Immune System. Function. - protect the body from infection by microorganisms. - assists in healing. - removes or repairs damaged cells. - identifies self from non-self. - recognizes and eliminates host cells that have been altered by viruses or cancer.

E N D
Function • - protect the body from infection by microorganisms. • - assists in healing. • - removes or repairs damaged cells. • - identifies self from non-self. • - recognizes and eliminates host cells that have been altered by viruses or cancer.
Cells of the Immune Response WBCs control the immune response, including: • neutrophils, • eosinophils, • basophils, • monocytes, and macrophages, and • the B and T lymphocytes. Platelets also play a role in healing.
Neutrophils, Eosinophils, and Basophils (granulocytes) contain enzymes that break down and destroy MO and digest cellular debris, then die. • - The neutrophils(40-70%)are the first WBCs to arrive at an area of injury or infection . • - Eosinophils(1-3%) are involved in the allergic response and are important in the defense against parasitic infections. • - Basophils(0.5-1%) release histamine and serotonin which increase capillary permeability. It secretes the natural anti-clotting substance Heparin, and are also involved in producing allergic responses.
Monocytes(3-7%) and Macrophages Monocytes are not phagocytic, but after several hours in the tissues, they mature into macrophages which are large cells capable of ingesting large quantities of cell debris and bacteria. The monocyte-macrophage cell system is called the reticuloendothelial system. • Lymphocytes(T &B) 30%of WBC - Produced in the bone marrow. - B cell ,after maturation in bone marrow, circulates in the blood in an inactive state and becomes a plasma cell that produce antibodies against the molecule that activated it ( humoral or antibody-mediated immunity).
- T lymphocytes(cellular immunity) matures through the thymus gland. Like a B cell, the mature T cell stays inactive until it encounters the specific molecule to which it has been programmed. The T cell may also release chemicals that alert B cells to the presence of the invader, thereby initiating a humoral response. T cells can stimulate (helper) or inhibit (suppressor) the inflammatory responses via the release of pro- or anti-inflammatory peptides known as cytokines. T cells are important for recognizing and destroying parasites and viruses that hide intracellularly, where the B cells are unable to encounter them. • The natural killer (NK) It is a cell that react to foreign molecules, but do not demonstrate specificity.
Platelets are not cells, but cytoplasmic fragments from specialized cells in the bone marrow called megakaryocytes. Once the platelets arrive at the site of injury, they adhere to the vessel wall, forming aggregates or plugs and release several biochemical mediators, including serotonin and histamine, which temporarily decrease blood flow and bleeding. Platelets circulate in the blood for about 10 days before they become non-functioning and are phagocytized by neutrophils and monocytes. If a person has too few platelets, he is at increased risk of developing multiple small hemorrhages .
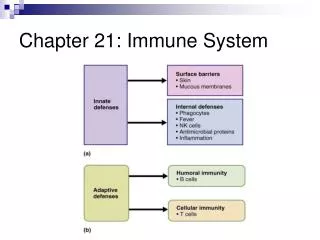
The Specific and Innate Immune Responses - Specific immune responses are specific and memory cell still remember the antigen. - innate immune response are non specific and no memory, but they are fast and effective. • Antigens An antigen is any molecule that can stimulate a specific immune response against itself or the cell that carries it. Billions of B and T lymphocytes are produced during fetal development with the potential to bind to at least 100 million distinct antigens • B-Lymphocyte Response to an Antigen When a B lymphocyte encounters its specific antigen, it differentiate into a plasma cell and memory cells. The plasma cell in turn begins to secrete millions of molecules of antibodies specific against that antigen. Once produced, the antibodies, also called immunoglobulins, circulate throughout the bloodstream seeking to eliminate the antigen that stimulated their production.
Immunoglobulins/Antibodies There are five specific immunoglobulins produced in response to an antigen: -IgG is the most common ( 80%), can crosses the placenta ,increases slowly during the primary (first) exposure to an antigen,but increases immediately and to a much greater extent with a second exposure -IgMantibody is produced first and in highest concentration during the primary exposure to an antigen. IgM is the largest antibody in size.
-IgA antibody is most concentrated in secretions such as saliva, vaginal mucus, breast milk, gastrointestinal (GI) and lung secretions, and semen. IgA acts locally rather than through the systemic circulation. Maternal IgA passes to an infant during breastfeeding . -IgE is responsible for allergic reactions. It is also the antibody most stimulated during a parasitic infection. -IgD exists in low concentration in the plasma. Its role is unclear.
The Role of the T Cell in B-Cell Response to an Antigen To mount an antibody attack against a microorganism, T cell support is almost always required. As described below, cytokines released by activated T lymphocytes trigger B cell proliferation and differentiation into antibody-secreting plasma cells. Memory Cells Some B lymphocytes do not become antibody-secreting plasma cells after antigenic stimulation, but rather become memory cells. Memory cells circulate indefinitely in the blood and become active immediately upon repeat exposure to the antigen.
The first time a B lymphocyte is exposed to its antigen (the primary exposure), production of antibodies against the antigen can take 2 weeks . Normally antibodies to an antigen are detectable in the blood within 3 to 6 months. Because of memory cells, the next time the antigen is encountered, the antibody response occurs almost immediately (secondary immune response ) .
T-Lymphocyte Response to an Antigen When a T lymphocyte binds to an antigen, it is stimulated to mature and reproduce. This reproduction results in up to four subtypes of T cells capable of acting in response to the antigen: cytotoxic T cells, helper T cells, regulatory T cells, and memory T cells. The T-cell response to antigen is called a cell-mediated response, because the T cells respond directly; they do not need to become plasma cells and secrete antibody to destroy the antigen. - Cytotoxic T cells directly destroy the antigen by releasing toxic chemicals. These chemicals punch holes in the membranes of the cells carrying the foreign antigen.
- Helper T cells secrete peptides, called cytokines, which act as cell messengers to coordinate the response of cytotoxic T cells and B cells. - Regulatory T cells act to suppress the host's immune response, a function which under some circumstances may increase the risk of infection, but under other circumstances may serve to protect the host . - Memory Tcells circulate in the bloodstream until the specific antigen that timulated their production is encountered again. Subsequent responses to that antigen occur rapidly.
Self-Antigens Each individual possesses cell surface antigens that are unique to that individual. These antigens, serve as a sort of cellular fingerprint. Development of Self-Tolerance During gestation, hundreds of thousands of T and B cells are formed. Some of these T and B cells fit lock and key with host antigens and are therefore capable of reacting against them. To eliminate the potential of attack against host cells, T cells residing in the thymus and B cells in the bone marrow are exposed during a critical period of embryogenesis to a multitude of host antigens.
If, during this time, a B or T cell encounters an antigen to which it matches, the B or T cell is programmed to undergo self-destruct. This leaves behind only cells tolerant to host antigens. This theory of tolerance is called the clonal deletion theory, because it explains the elimination of clones of immune cells that react with self-antigens.
Immune and Inflammatory Deficiencies Immune and inflammatory deficiencies inhibit the body's ability to respond to infection or injury, and may result from impaired function of any or all white blood cells. Complement or coagulation proteins may also be deficient. Immune and inflammatory deficiencies may be congenital or acquired after illness, infection, or prolonged stress. The deficiencies may be temporary or permanent.
Congenital Immunodeficiency It occurs as a result of a genetic defect. It may involve: - one type of T or B cell, all the T cells , or all the B cells . - one immunoglobulin (usually IgA or IgG). With total B-cell deficiency, the missing immunoglobulins can be provided to the individual by intravenous administration. Infants with primary T-cell deficiency have severely impaired ability to fight infection because T cells are required not only for cellular immunity but humoral immune responses as well.
If the bone marrow stem cells are dysfunctional, T and B cells and all other white blood cells may be deficient.This condition is called severe combined immunodeficiency syndrome (SCIDS). It is fatal in • early childhood. Acquired Immunodeficiency It is reduced functioning of the immune system developing after birth. It may arise in response to: - infection, malnutrition, chronic stress, or pregnancy. - systemic illnesses such as diabetes, renal failure, and cirrhosis of the liver.
- receiving corticosteroids to prevent transplant rejection or to reduce chronic inflammation - receiving chemotherapy and radiation. - Surgery and anesthesia may also depress the immune system. *Acquired immunodeficiencies can be of B or T cell function, or both. Because B cells require helper T cell stimulation to successfully fight infection, T cell deficiencies also cause dysfunction of the humoral immune system.
Consequences of Immunodeficiency Immunodeficient individuals repeatedly develop frequent severe and unusual infections and are often unable to fight them. - Individuals with T-cell deficiencies frequently develop viral and yeast infections. - Individuals with B-cell deficiencies are especially susceptible to infections by bacteria. - HIV destroys the helper T cells and infects other white blood cells.
Conditions of Disease or Injury 1-Allergy An allergy is an overstimulation of inflammatory reactions that occurs in response to a specific environmental antigen. An antigen that causes an allergy is called an allergen. Allergic reactions may be antibody mediated or T cell mediated. Cause of Allergies The cause of allergies is unclear, although there appears to be a genetic predisposition.
Clinical Manifestations - Localized swelling, itching, and redness of the skin, with skin exposure to an allergen. - Diarrhea and abdominal cramps, with exposure to a gastrointestinal allergen. - Allergic rhinitis, characterized by itchy eyes and runny nose, with exposure to a respiratory allergen. Diagnostic Tool - Skin tests help in diagnosing an allergy. A small amount of the suspected allergen is injected under the skin. Individuals allergic to that allergen will respond with marked erythema, swelling, and itching at the injection site. - Serum immunoglobulin analysis may indicate increased basophil and eosinophil count.
Complications • A naphylaxis, which is characterized by a decrease in blood pressure and closure of the airways. • Without intervention, severe reactions can lead to cardiovascular shock, hypoxia, and death. Treatment • Antihistamines • Corticosteroids, inhaled, administered nasally, or taken systemically. • Desensitization therapy, involving repeated injections of small amounts of an allergen to which an individual is sensitive.
3-Acquired Immunodeficiency Syndrome AIDS Is caused by the human immunodeficiency virus (HIV).There are at least two HIV viruses,HIV-1 & HIV-2. • The Course of HIV Infection - May remain asymptomatic for 8 or more years. - Once the virus begins destroying helper T cells, it will progress rapidly, usually over the course of 2 to 5 years. - It should be emphasized that HIV infection is not AIDS, and occasionally an individual infected by the virus will survive more than 12 years with no signs of AIDS. - However, infection with the virus means the individual is contagious to others, whether symptoms of AIDS are present or not.
Passage of HIV • HIV is passed between individuals during the exchange of body fluids, including blood, semen, vaginal fluid, and breast milk. • Urine and gastrointestinal contents are not believed to be a source of HIV transmission unless they visibly contain blood. • Tears, saliva, and sweat may contain the virus, but in quantities thought to be too low to cause infection. • Individuals at Risk of Developing HIV The individual's immune, nutritional, and general health status, the amount of virus to which the individual is exposed & the age and sex of an individual are factors that influence risk.
Spread to Women and Children • - Women are more susceptible than men to infection during heterosexual intercourse because of the normal microscopic vaginal tears and bleeds that occur with intercourse. In addition, infected semen remains in the woman's vagina up to 48 to 72 hours longer than the amount of time the penis is exposed to vaginal secretions. • - A woman infected with HIV may pass the infection on to her infant across the placenta, usually during the third trimester, or after exposure of the infant to contaminated blood and amniotic fluid during the birth process. An infant born to an untreated, infected mother has at least a 25% chance of becoming infected with the virus.