Download
1 / 55
610 likes | 1.74k Views
Spinal Stenosis / Neurogenic Claudication. Chris Dowding Half Day Feb 16 2012. Low Back Pain. About ¾ of all individuals will experience low back pain at some time in their lives; usually, it resolves in a matter of weeks.

E N D
Spinal Stenosis/NeurogenicClaudication Chris Dowding Half Day Feb 16 2012
Low Back Pain • About ¾ of all individuals will experience low back pain at some time in their lives; usually, it resolves in a matter of weeks. • Low back pain is the leading cause of disability in people younger than 50 years of age. • LBP - M=F • Peak incidence between 35 and 50 years of age • Primary causes of low back pain • Muscle strain or ligament sprain • Facet joint arthropathy • Discogenic pain or Annular tears • Spondylolisthesis • Spinal stenosis
What is Spinal Stenosis? • First described by Verbiest 1954 • 7 patients with syndrome of the following: • Lumbar canal narrowing • Neurogenic spinal claudication • Radicular pain • Motor weakness in lower limb
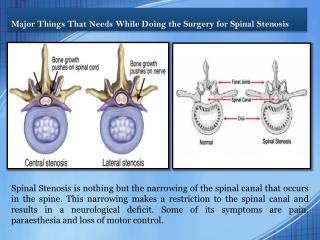
Definition • Spinal Stenosis • Narrowing of the spinal canal, resulting in a clinical syndrome of leg dominant pain • Primary subtypes • Central canal stenosis • Subarticularstenosis (area under facet joints) • Neural foramina stenosis • Symptoms are caused by compression of the nerve roots • Results in neurogenicclaudication
Definition • Neurogenicclaudication • Discomfort or pain that radiates from the spinal area into the buttocks and frequently into thigh and lower leg
Etiology • Spinal Stenosis • Narrowing of spinal canal due to: • Degenerative • (most common) • Developmental • Congenital disorders • Post traumatic • Steroids • Post-surgical • Certain disorders
Degenerative Stenosis • Narrowing is secondary to arthritis • Typically following order • Disc degeneration • Facet osteoarthritis • Flavum hypertrophy • Symptoms develop around 60 yo
Intervertebral Joints Two Components: 1. Outer rim of fibrocartilage called the annulus fibrosus (attaches to cartilaginous end plate) • Connects vertebral bodies in a fibrocartilaginous joint (no capsule, little motion) 2. Facet (Zygapophyseal) joints
Intervertebral Disks • Fibrocartilaginous • Collagen, water, Proteoglycans • Annulus Fibrosus • Obliquely oriented collagen • Type I collagen • Outer rim contains free nerve endings • Central Nucleus Pulposus • 88+% water, high polysaccharide content • No blood vessels or nerves • Type II collagen
Intervertebral Disks • Function • spinal motion and stability. • Disk is avascular. • Nutrients fluid via diffusion through pores in the hyaline cartilage end plates • As Disks ages • Decreased water content, increased collagen.
Disk Degeneration • Begins roughly third decade of life. • Characterized by a decline in proteoglycan concentration with resultant loss of hydration and a decreased number of viable cells • L4-5 and L5-S1 are the disks that typically degenerate first
Degenerative Disks • Disk height decreases, resulting in alteration of the segmental spinal biomechanics • Increasing wear on facet joints • The precise cause(s) of disk degeneration are unclear, and there are several potential contributors • Comorbidities like diabetes, vascular insufficiency, and smoking are potentially associated with disk degeneration • There appears to be a genetic component to disk degeneration
Degenerative Stenosis • Loss of disc height • Infolding of flavum • Increased stress across facets • Facet OA and hypertrophy • Osteophytesand capsule thickening • Cysts
Degenerative Stenosis • Spondylolithesis (+/- spondylolysis) • Can result in stenosis • Back pain is primary symptom • Neurogenicclaudication is secondary
Developmental Stenosis • Narrowing of canal due to growth disturbance of posterior elements • Congenitally short pedicles • Often present in 20’s
Presentation • Constellation of symptoms • Leg pain • Difficulty ambulating • Comfortable sitting • Pain with prolonged walking • Neurologic deficits
History • Age • Pain • Location • Timing • Characteristics • Aggravating or relieving factors? • Previous therapy? • PMHx • Social History/Occupation • Meds/Allergies • Functional Inquiry • How far can you walk? • Can they bike?
Red Flags Night sweats Fever Weight loss Bowel/Bladder History of cancer Immunosuppression Saddle anaesthesia Sexual dysfunction Age > 60 History of IVDU Chronic infections Rest/night pain
Physical Exam • Vitals • Inspect • Gait • Leg length • Trendelenburg test • Spinal alignment • Palpate • Spinous processes • Paraspinal muscles • Greater trochanters
Physical Exam • ROM • Spine flexion, extension, rotation, lateral bend • Hip flexion, extension, rotation • Pain with etxension, relieved by flexion • Neuro • Strength • Sensation • Reflexes • Half of patients with symptomatic stenosis have motor or sensory deficits • Usually mild
Special Tests • Romberg maneuver • Patient stands with eyes closed • Look for unsteadiness, wide based stance • Indicates damaged proprioception
Imaging • Lumbar x-rays • +/- spondylolithesis • Extent of disc narrowing • Foramina osteophytes • CT/MRI • Can illustrate reductions in cross sectional diameter of central canal or foramina • Useful for pre-op planning or assessing candidacy for epidural injections • Large number of people may have radiologic findings but are asymptomatic
Location of stenosis • Centrally • Lateral recess & neural foramina • Degeneration of • Disk • Facets (hypertrophy) • Synovial cysts • Joint capsule • Thickening of ligamentumflavum • Osteophytes
Identifying the cause • Differential is broad • Some non-spinal causes to keep in mind • Vascular claudication • Hip arthritis • Diabetes (peripheral neuropathy)
Vascular Claudication • Cramping/tightness in calf • PVD (skin ulcers, trophic changes) • Diminished pulses • Relieved by cessation of activity • Versus neurogenic (flexion or sitting down) • Capable of activity while flexed • shopping cart • Cycling • walking uphill
Hip Arthritis • Groin pain • Referred pain in thigh • increased with activity • Internal rotation diminished • XR - OA
Diabetes Glove & stocking distribution Not affected by activity level
Conservative Management • Physical therapy • Abdominal strengthening • Biking • Brace/corset • Slight lumbar flexion • Limit hours worn per day • Avoid atrophy • Pain pyramid • Tylenol • NSAIDS • Narcotics
Conservative Management • Epidural injections • Theory is that compression of nerve roots causes inflammation and thus symptoms • Cortocosteroids to reduce inflammation • Evidence is not convincing one way or another • Although this practice is increasing
Natural History? • Natural course of disease • Pain / function of patients with lumbar stenosis • remains unchanged in majority patients • After one year of non-op management the majority of patients will be neither worse nor better • Rapid decline uncommon • Therefore prophylactic treatment non indicated • Improvement is also uncommon • If patient is miserable at baseline, non-op management may not be appropriate
Surgical indications Progressive neurologic deficit Intractable pain Persistent impairment and functional limitation Confirmation by imaging LBP is not alleviated with surgery!
Lumbar Stenosis:So when should we operate? • Goals of surgery • Decompress central canal and neural foramina • Options • Laminectomy ** • Partial facetectomy ** • Lumbar arthrodesis • +/- Instrumentation • Interspinous distraction • MIS
Algorithm? Edward N. Hanley Jr., MD, Spinal Stenosis, Charlotte
Treatment – Spinal Stenosis • Maine lumbar spine study • 119 patients • 67 treated surgically • 52 treated nonsurgically • After 4 years 70% of surgically treated and 52% of nonsurgically treated reported that their predominant pain was better. • Satisfaction 63% of surgically treated and 42% of nonsurgically treated. • Atlas et al. Spine. 2000.
Malmivaara2007 • Design • RCT • 4-university hospitals • 94 patients • Surgical • Laminectomy 10 patients also had transpedicular fusion • Outcome • Oswestry Disability Index (0-100) • Intensity of pain (0-10) • Walking ability – self-reported • 6,12&24 months
Malmivaara2007 • Inclusion Criteria • Back pain radiation to lower limb/buttock • Fatigue loss sensation aggravated by walking • Persistent pain without progressive neurologic dysfunction • SAC (sagital) < 10 mm • Duration of symptoms > 6 months • Signs & symptoms correspond to segmental radiographs • Severity of disease to justify surgical/non-surgical rx
Malmivaara2007 • Exclusion • Severe LSS intractible pain • Progressive neurologic dysfunction • Mild LSS with clinical signs feeble enough to exclude surgical treatment • Spondylolysis and spondylolytic disease • Earlier back operation due to stenosis • Herniated disc during last 12 months • Another spinal disorder • Intermittent claudication due to PVD • Severe OA of L/E • Neurologic disease with impaired function of L/E • Psych • Alcoholic
Malmivaara2007 • Randomization: • Central office computer generated blocks variable size for each hospital • Physician phoned central office after baseline exam, questionnaire completed
Malmivaara2007 • Intervention • Surgical group • Segmental decompression • Facetectomy • Instability treated at surgeon discretion • Fusion of lumbar spine +/- instrumentation • Degenerative listhesis warranting procedure • Brochure for nature of disease, symptoms and activities • Non-operative group • Physiatrist followed throughout • Physiotherapist followed • Exercises • Brochure for nature of disease, symptoms and activities
Malmivaara2007 • Walking ability • Reported & measured • No significant difference between 2 groups
Malmivaara2007 • Conclusion • Those undergoing surgery reported greater improvement over non-operative treatment • Benefit diminished over time • Issues • Longer f/u needed • Surgical treatment differed • Selected bias from exclusion criteria • Screened for those who may benefit from surgery
Weinstein 2008 • SPORT Trial • “Surgical versus Nonsurgical Therapy for Lumbar Spinal Stenosis” • Inclusion • 12 weeks of symptoms typical to stenosis • Exclusion • Spondylolithesis
Weinstein 2008 • 2 cohorts • A) randomization • Op vs non-op • B) observational • Elective op vs. elective non-op • Outcomes • Bodily pain and physical function • SF-36 • Modified Oswestry disability index • 6 weeks, 3 months, 6 months, 1 year, 2 years