Download
1 / 44
440 likes | 800 Views
Treatment options for Lumbar Spinal Stenosis. Gary Jones, SPT; Megan Ivy, SPT; Jill Kloesel , SPT; Chris Rogers, SPT; & Chris Zoch , SPT. Search Strategy: 3/2/09 - 3/4/09. Database: PubMed Search Terms: lumbar fusion, degenerative; Journal: Spine, Author: Deyo

E N D
Treatment options for Lumbar Spinal Stenosis Gary Jones, SPT; Megan Ivy, SPT; Jill Kloesel, SPT; Chris Rogers, SPT; & Chris Zoch, SPT
Search Strategy: 3/2/09 - 3/4/09 • Database: PubMed • Search Terms: • lumbar fusion, degenerative; Journal: Spine, Author: Deyo • lumbar spinal stenosis, long-term outcomes; Journal: Spine • lumbar spinal stenosis, outcomes • lumbar spinal stenosis, nonoperative • epidural steroids AND lumbar stenosis • epidural blocks AND lumbar stenosis • acupuncture AND lumbar stenosis • epidural injections AND lumbar stenosis AND complications • lumbar spinal stenosis, physical therapy • Database: Medline & CINHAL via Ebsco Host • Search Terms: • lumbar stenosis • lumbar stenosis AND physical therapy
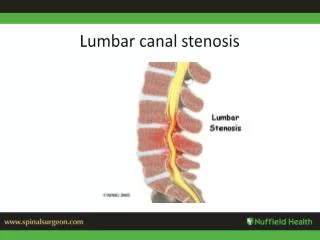
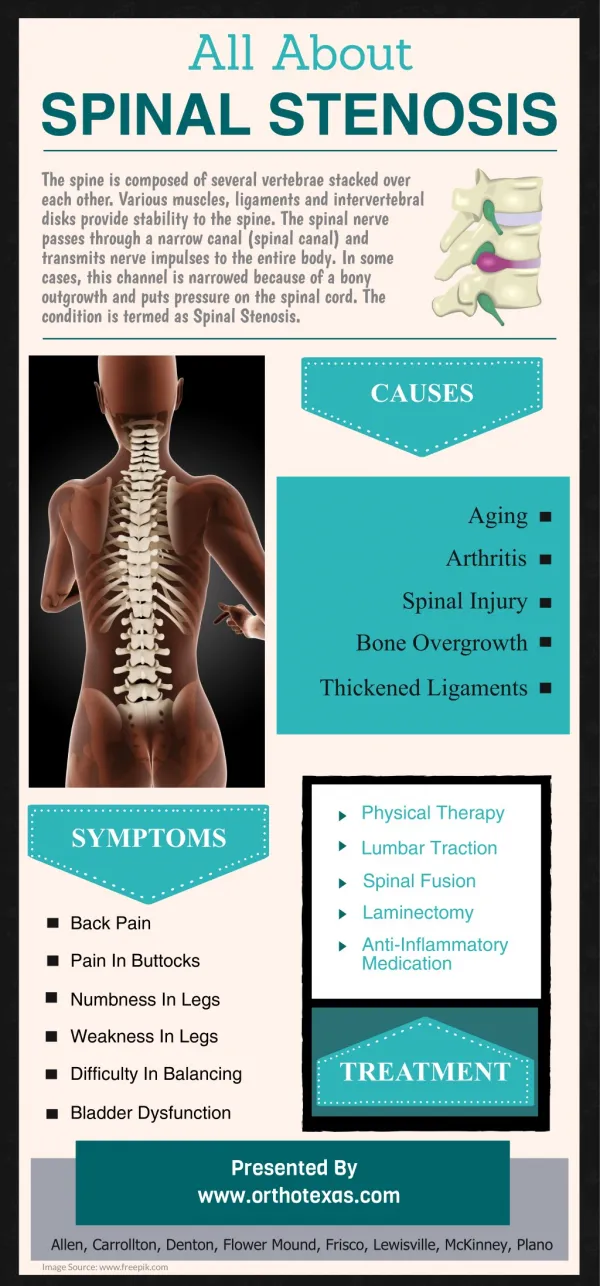
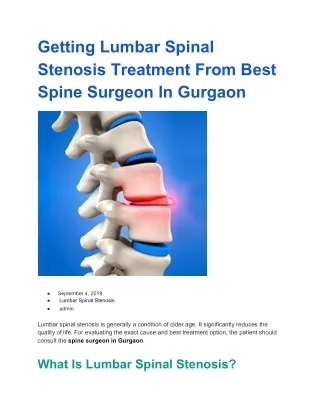
LSS Definition • Stenosis – from Greek root – narrow • Any narrowing of Lumbar : • Spinal Canal (Central Stenosis) • Interverterbral Canal (Lateral Stenosis)
Central Stenosis- Causes (Fritz 1998) • Facet joint arthrosis & hypertrophy • Ligament flavum, thickening or bulging • IV Disc bulging • Spondylolesthesis (http://www.eorthopod.com/public/patient_education/6569/lumbar_spinal_stenosis.html)
Lateral Stenosis – Causes (Fritz 1998) • Facet joint hypertrophy • ↓ disc height • Posteriolateraldisc bulge • Spondylolesthesis ( http://www.svmh.com/spine/causes_mechanical.asp)
LSS Etiology Base Classification (Fritz 1998) • Primary Stenosis • Congenital malformation • Postnatal development of SC • < 9% of cases • Secondary Stenosis • Acquired condition • Usually from degenerative changes • Also from: • Surgical scarring • Tumor, infection, • Fx, systemic bone disease
LSS: Clinical Presentation (Fritz 1998) • ↑ age • Long Hx of LBP • 90% with leg pain • more recent than LBP • May have: • radicular pain • Sensory, motor, reflex changes • LE symptoms may be: • Uni or bilateral • ≈50% have +SLR • ↓ROM esp. extension • Aggs: extension, WB • Eases: flexion, NWB • Neurogenicclaudication in ≈ 60% • Often reason for seeking care
LSS: Natural History (Fritz 1998) • Common view: • Fixed anatomic pathology • Poor natural history • Responsive to surgical intervention • Studies suggest: • Deterioration not inevitable • Many patients improve or unchanged with time
Treatment Options • Physical Therapy • Mob/Manip • Traction • Aquatics • Therapeutic Ex • Unloaded TM Walking • Modalities • Nerve Glides • Etc. • Acupuncture • Injections • Facet • Epidural • Nerve Block • Surgery • Laminectomy • Fusion • Etc, etc, etc . . .
A comparison between two physical therapy treatment programs for patients with lumbar spinal stenosis: A randomized clinical trial. Whitman JM, Flynn TW, Childs JD, et al. Spine. 2006 • First RCT comparing non-surgical TX for LSS • N=56 • Comparison: • Manual Therapy, Exercise, BWS Treadmill Walking • MPTExWG • Flexion Exercises, Treadmill Walking • FExWG
Results • Perceived Recovery • Sig diff @ 6wks (p=0.0015) • 79% v 41% • Contiued diff @ • 1yr • Longterm FU
Results • 2 Outcome Measures- not validated w/ LSS pt • ODI, NPRS, SSS, Walking tolerance test • All favored MPTExWG • Healthcare Utilization –MPTExWG
A non-surgical approach to the management of lumbar spinal stenosis: A prospective observational cohort studyMurphy DR, Hurwitz EI, Gregory AA, & Clary R; BMC Musculoskeletal 2006 • 57 patients • PT focusing on Distraction Manipulation (DM) and Neural Mobilization (NM) combined with Exercise • ‘cat & camel’, nn flossing, stabilization, etc. • Outcome Measures • Roland-Morris Disability Questionnaire (RM) • Three Level Numerical Rating Scale (NRS) • Patient Perceived Percentage Improvement • Baseline, D/C, & Long Term Follow-up (16.9 mos)
Neural Mobilization Intraneural edema
Results • 2 subjects went on to require surgery • 2/3 → clinically meaningful difference
Nonsurgical management of patients with lumbar spinal stenosis: a literature review and a case series of three patients managed with physical therapyWhitman JM, Flynn T, Fritz J- 2003 • 3 subjects –> 18 month period • Retired military • 5 sessions • Rotational & PA mobilization/manipulation • Addressed hip mobility & ↓ extension • PA accessory motion mobilization • Rectus femoris/iliopsoas stretching • Gluteal/lower abdominal strengthening • Pts 2 & 3 also received BWS treadmill ambulation
Results • Compared to baseline . . . • ↓ pain with activities that previously caused pain • Able to ambulate further • ↑ activity, ↑ sleep • Oswestry showed significant results
SPORT Trial Surgery vs Nonsurgical Therapy for Lumbar Spinal Stenosis Weinstein, Tosteton, Lurie et al. • Author’s Conclusions • Limitations • Our Conclusion
Epidural Steroid Injections • Pain Physician Study • 65% of pts showed improvement at 6 weeks • 62% at 6 months • 54% at 12 months • Assessed by ODI, Standing/walking tolerance tests, VAS, & Pt Satisfaction • Possibly helpful for short-term relief
Epidural Steroid Injections • Problem: Statistical significance vs. Clinical • Generally low risk, though cases of thromboembolic stroke have been related to procedure • Must consider patient Hx • Combination with PT? • Whitman et al, 2006: “combining ESI & PT may be promising”
Nerve Block Injections • Caudal epidural injection of anesthetic at affected level • Journal of American Geriatric Society Study • Pain ↓ from 3.43 +/- 0.82 to 1.5 +/- 0.86 with results lasting 4-10 months • Roland 5-Point Pain Scale • More severe cases → less improvement • Clinical implications similar to steroid injections
Acupuncture • Evidence inconsistent at this time • Very few studies specific to stenosis • One small Japanese study showed slight alleviation of symptoms following electroacupuncture stimulation of the pudendal nerve • Ouch!
Spine Surgery: Epidemiology • Increased 220% from 1990 to 2001 and is still increasing further • The rate grew exponentially in 1996 with the FDA approval of intervertebral cages
Surgery: Epidemiology • LSS is generally treated with vertebral fusion and/or a laminectomy • The rates of fusion increased in 1990-1991 by 29% and from 2000-2001 by 51%
The Evidence? • So lets say Evidence = Bungee Cord Wouldn’t you want to check first?
The Evidence for Surgery • We know lumbar fusion with the use of IV cages is one of the most rapidly increasing major surgical procedures • in addition to being one of the most expensive • Yet there is scant evidence supporting fusion or the use of IV cages as an effective treatment for LSS • Most evidence is old and is not very supportive • There is little new evidence either
The Evidence for Surgery • So lets see what evidence there is…
The Maine Lumbar Spine Study • Series of four articles from 1996 to 2005 • For ~ 10 years they compared outcomes of surgical vs. non-surgical treatment for LSS • Authors found some benefits to surgery for LSS Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the maine lumbar spine study. Spine. 2005;30(8):936.
The Maine Lumbar Spine Study • Outcome Measures: • back pain • leg pain • predominant symptoms compared to baseline • and whether they would choose the same tx • Taken at 1 year, 4 years, and finally at 8-10 years
Results • Found that patients with surgery had reduced leg pain at 8-10 years • Also found that surgery tends to favor better short term outcomes (1-4 years) than non-surgical treatment • However, we do have a few concerns . . .
What the data really means… • Lets take a closer look at these results: • The non-surgical group consisted of many different treatment strategies • To name a few spinal manipulation, traction, and even bed rest! • So is it very objective to group all non-surgical approaches as one model for treatment?
What the data really means… • Short term benefits to surgery? • In their evaluation of 1 year outcomes, the authors noted that the non-sx group was more than 2X as likely to be on worker’s compensation. • Potential bias in these patients reporting results?
What the data really means… • Lets also note that the outcomes were measured with qualitative scales such as (improved, same, worse)
What the data really means… • The results showed less leg pain in sx patients for 8-10 years (p = 0.04) • BUT there is a caveat in there data for leg pain • The result was considered “improved” if the patient said “completely gone” and “better,” but also included “a little better” or “about the same” • Is it appropriate to associate minimal or no effect from treatment with improvement?!
Are we being fooled? • What’s wrong with this statement? “…82% of patients treated surgically would still definitely or probably choose their initial treatment compared with 64% of those treated non-surgically (P = 0.05).” • They use nondescript terminology like “probably” because they cannot claim significance with p = 0.05, must be p<0.05
Conclusion? • So with all these limitations in mind, can we agree with the authors conclusions? • And if we do, the only long-term benefits were reduced leg pain and some relative short term benefits • Also an observational non-random design
Other Evidence • Quality pro-surgery evidence for LSS was not to be found, at least not in the U.S. • One Japanese study found favorable benefits for surgery Miyamoto H, Sumi M, Uno K, Tadokoro K, Mizuno K. Clinical outcome of nonoperative treatment for lumbar spinal stenosis, and predictive factors relating to prognosis, in a 5-year minimum follow-up. Journal of Spinal Disorders & Techniques. 2008;21(8):563.
Other Evidence • Maintains that specific patients with LSS were appropriate for surgery and others with non-surgical methods. • Similar concept to subgrouping LBP patients for traction, manipulation, etc…
Other Evidence • “ the current study demonstrated that the response to initial non-operative treatment was a statistically significant factor for a good prognosis. That is, it has been demonstrated that non-operative treatment should be the treatment of first choice for LSS…”
More Evidence • Study advocates surgery (laminectomy or fusion) • But only shown beneficial in short term (2 years max) • “…we propose that surgical decompression should be suggested with caution and only after due conservative treatment of the patient.” Malmivaara A, Slätis P, Heliövaara M, et al. Surgical or nonoperative treatment for lumbar spinal stenosis?: A randomized controlled trial. Spine. 2007;32(1):1.
Final Thoughts • PT is beneficial in stopping and/or reversing symptoms of LSS • Manipulation/Mobilization, Therapeutic Exercise, BWS Treadmill Walking, Hip flexibility • Surgery is invasive, expensive, dangerous and lacks substantial evidence • May be effective in severe cases • Many other options have little to no concrete evidence • Initial conservative treatment does not effectpossible future surgical outcomes • Lack of Research
References • 1. Amundsen T, Weber H, Nordal HJ, Magnaes B, Abdelnoor M, Lilleas F. Lumbar spinal stenosis: Conservative or surgical management?: A prospective 10-year study. Spine. 2000;25(11):1424-35; discussion 1435-6. • 2. Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE. Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the maine lumbar spine study. Spine. 2005;30(8):936. • 3. Botwin KP, Gruber RD, Bouchlas CG, et al. Fluoroscopically guided lumbar transformational epidural steroid injections in degenerative lumbar stenosis: An outcome study. American Journal of Physical Medicine & Rehabilitation. 2002;81(12):898. • 4. Ciocon JO, Galindo-Ciocon D, Amaranath L, Galindo D. Caudal epidural blocks for elderly patients with lumbar canal stenosis. J Am Geriatr Soc. 1994;42(6):593-596. • 5. Deyo RA, Gray DT, Kreuter W, Mirza S, Martin BI. United states trends in lumbar fusion surgery for degenerative conditions. Spine. 2005;30(12):1441. • 6. Fritz JM, Delitto A, Welch WC, Erhard RE. Lumbar spinal stenosis: A review of current concepts in evaluation, management, and outcome measurements. Arch Phys Med Rehabil. 1998;79(6):700-708. • 7. Inoue M, Hojo T, Nakajima M, Kitakoji H, Itoi M, Katsumi Y. Pudendal nerve electroacupuncture for lumbar spinal canal stenosis-a case series. ACUPUNCTURE IN MEDICINE. 2008;26(3):140-144. • 8. Linn AJ, DeSilva C, Peeters-Asdourian C. Thromboembolic stroke: A rare complication associated with peri-procedural management of an epidural steroid injection. Pain Physician. 2009;12(1):159-162. • 9. Malmivaara A, Slätis P, Heliövaara M, et al. Surgical or nonoperative treatment for lumbar spinal stenosis?: A randomized controlled trial. Spine. 2007;32(1):1. • 10. Miyamoto H, Sumi M, Uno K, Tadokoro K, Mizuno K. Clinical outcome of nonoperative treatment for lumbar spinal stenosis, and predictive factors relating to prognosis, in a 5-year minimum follow-up. Journal of Spinal Disorders & Techniques. 2008;21(8):563. • 11. Murphy DR, Hurwitz EL, Gregory AA, Clary R. A non-surgical approach to the management of lumbar spinal stenosis: A prospective observational cohort study. BMC Musculoskeletal Disorders. 2006;7(1):16. • 12. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med. 2008;358(8):794. • 13. Whitman JM, Flynn TW, Childs JD, et al. A comparison between two physical therapy treatment programs for patients with lumbar spinal stenosis: A randomized clinical trial. Spine. 2006;31(22):2541. • 14. Whitman JM, Flynn TW, Fritz JM. Nonsurgical management of patients with lumbar spinal stenosis: A literature review and a case series of three patients managed with physical therapy. Physical Medicine & Rehabilitation Clinics of North America. 2003;14(1):77-101.