Developing a Platform for Learning
Developing a Platform for Learning Changing the Culture of Patient Safety amongst Junior Medical Staff. Introduction


Developing a Platform for Learning
E N D
Presentation Transcript
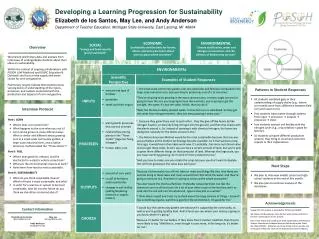
Developing a Platform for Learning Changing the Culture of Patient Safety amongst Junior Medical Staff Introduction Junior doctors commonly make mistakes which may compromise patient safety. Explanations for this include overworking, lack of support and inexperience. There have already been extensive attempts to address the former, but inexperience will always exist. In fact, a large part of gaining experience is learning from mistakes. Despite the NHS’ recent push to encourage a “no blame” culture, making mistakes can still be viewed as a shameful, embarrassing and demoralising event, not to mention the guilt and fear that comes with it. The current model for learning from mistakes means that junior doctors only really learn from their own. I made an identity error which resulted in a patient receiving an unnecessary blood transfusion. Despite this being a ‘near miss’ (the patient appears not to have suffered any harm), I have never felt so awful in my life. Only five months earlier I had taken the Hippocratic Oath “to do no harm” and I was already making potentially harmful mistakes. I felt ashamed, mistrustful of my ability and alone. Fig 1. Fig 2. Fig 3. Fig 1: Types of mistakes made by % of FY1s and quantity. Fig 2: Breakdown of mistakes made over first 20 weeks. Fig 3: Identifying the problem Methods and Objectives I designed a survey for all the Foundation Year 1s at Yeovil District Hospital to better understand the culture surrounding mistakes, and the types of mistakes that were being made. Using the results of the primary survey and the support of senior staff I have introduced a “Near Misses” session for FY1’s once a month in which we discuss mistakes that have been made, with a consultant present to facilitate. The aims of these sessions are to: A) Promote a culture of no blame B) Feedback some information to clinical governance C) Share learning experiences Conclusions 100% of FY1’s have made a mistake that could compromise patient safety. 63% discuss mistakes with colleagues, 44% with seniors and only 13% with their educational supervisor. Barriers to discussing mistakes included shame, embarrassment, fear of judgement and unapproachable seniors. 94% thought a “Near Misses” session would be useful. After the 3rd session 100% agreed the sessions were useful, 53% had changed their practise as a result of something they learned at the sessions. FY1’s do not formally report their mistakes. This project has identified a culture of fear surrounding making mistakes. If we do not report or discuss them then how can we learn from and act to prevent them in the future? Results and outcomes After discussing an error as a group we have made a number of recommendations to clinical governance regarding strategies to avoid repetition of mistakes. We have been invited to attend the “Safer medicines group” to discuss some of our recommendations. Examples of this include red allergy bands, writing the patients allergy status above their bed space, the use of near patient testing for INRs, routine appointment booking for post discharge follow up of patients on high risk medications, revision of warfarin charts to improve safety, additional teaching on warfarin prescribing and drug interactions and feedback from pharmacy about our common prescribing errors. There will be an FY1 on this committee from now on. In terms of sustainability, the “Near Misses” sessions are now established for the next cohort of F1s and we are initiating a parallel session for the foundation year two trainees. “You must promote and encourage a culture that allows all staff to raise concerns openly and safely.” GMC Good Medical Practice 2013 Discussion I believe this project has succeeded in effecting a cultural change surrounding the discussion of mistakes among junior doctors, from a culture of fear, to a culture of openness and ‘no blame’. The feedback I have received from the initial sessions has been overwhelmingly positive. The juniors have found the sessions cathartic and reassuring but the most satisfaction is derived from knowing that by discussing their errors, they may have prevented someone else repeating them. It is encouraging that many juniors have altered their practise as a result of something they learned at these meetings. Perhaps more importantly, by discussing their mistakes on a regular basis they are becoming conscientious, self-aware and self-improving practitioners, who will improve our health service in the years to come. Author: Dr Sinead Millwood Yeovil District Hospital Higher Kingston Yeovil BA21 4AT millwoodsinead@gmail.com