Download
1 / 22
220 likes | 362 Views
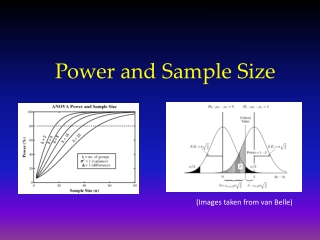
Equivalence and Bioequivalence: Frequentist and Bayesian views on sample size. Mike Campbell ScHARR CHEBS FOCUS fortnight 1/04/03. Equivalence. Many trials are not designed to prove differences but equivalences Examples : generic drug vs established drug Video vs psychiatrist

E N D
Equivalence and Bioequivalence:Frequentist and Bayesian views on sample size Mike Campbell ScHARR CHEBS FOCUS fortnight 1/04/03
Equivalence • Many trials are not designed to prove differences but equivalences Examples : generic drug vs established drug Video vs psychiatrist NHS Direct vs GP Costs of two treatments Alternatively – non-inferiority (one-sided)
Efficacy vs cost • For some trials (e.g. of generics) one would like to show similar efficacy at less cost • Thus can have an equivalence and a cost difference trial in one study
Motivating example • AHEAD (Health Economics And Depression) • Trial of trycyclics, SSRIs and lofepramine • Clinical outcome - depression free months • Economic outcome – cost • Powered to show equivalence to within 5% with 90% power and 5% significance (estimated effect size 0.3 and SD 1.0)
Bio-equivalence (diversion) • For bio-equivalence we are trying to show that two therapies have same action • Usually compare serum profiles by e.g. AUC • Often paired studies • FDA: 80:20 rule 80% power to detect 20% difference
Frequentist view • Impossible to prove null hypothesis • All we can do is show that differences are at most Δ • Choose Δ to be a difference within which treatments deemed equivalent • General approach – perform two one-sided significance tests of H0: μ1-μ2> Δ and μ1-μ2< -Δ If both are significant, then can conclude equivalence
Figure from Jones et al (BMJ 1996) showing relationship between equivalence and confidence intervals
CIs Assume sd s is known. Then 100(1-a)% CI to compare difference in means is where Treatments deemed equivalent if interval falls in -Δ to +Δ
Let τ = μA - μB Let η = Δ - zα/2 σλ (1) Maximal Type I error rate is (1) when τ=Δ Power is defined when (1) has τ=0 or
If treatment groups have same size, n, then required sample size is (2) • This is similar to testing for a difference • Except • Usually Δ is smaller than for a difference trial • We use β/2 rather than β
Problems with equivalence trials • Poor trials (e.g. poor compliance and larger measurement errors bias trial towards null) • Jones et al (1996) suggest using an ITT approach and ‘per-protocol’ and hope they give similar results!
Bayesian sample size (O’Hagan and Stevens 2001) • Analysis objective Outcome is positive if the data obtained are such that there is a posterior probability of at least ω that τ >0 • Design objective We require the sample size (n1,n2)be large enough so there is a probability of at least ψ of obtaining a positive result. The probability ψ is known as the assurance
Bayesian assumptions • Let prior expectation of (μ1,μ2)T be ma according to analysis prior and md according to the design prior • Let variances be Va and Vd for analysis and design priors respectively • Let be ( )T,the observed data • Let S be the sampling variance matrix (note this depends on n1 and n2)
Let Wa =Va-1 ,Ws=S-1 and V*=(Wa+Ws)-1 and a=(1,-1)T Under analysis prior Posterior mean of (μ1, μ2) is Normally distributed with expectation and variance
Under design prior Unconditional distribution of is Normal with mean and variance From which can get sample size calculation (See O Hagan and Stevens)
Frequentist interpretation If then the Bayesian methods for determining sample size agree with frequentist If Va-1 =0 – weak analysis prior –’vague’ prior If - strong design prior Vd=0
Bayesian equivalence (after O’Hagan and Stevens(2001) • Analysis objective: Outcome of study is positive if the upper limit of the (1-ω)% prediction interval for τ is < Δ (one sided) or upper and lower limits of prediction interval for τ are within ± Δ (two sided). • Design objective: Sample size is such that there is a probability of at least ψ of obtaining a positive result.
A modification of O’Hagan and Stevens suggests that for equivalence trials, a positive outcome occurs when Two-sided and One-sided Sample size also a modification of O’Hagan and Stevens
Parameters for non-inferiority ma - the analysis prior mean could be 0 md - the design prior mean could be 0
What if mdandVd>0 ?A weak design prior Then we have some information about the possible differences, so ‘proving’ the null hypothesis is difficult E.g. if we were 50% sure that δ>0, before the trial then cannot be 80% sure that δ=0 after the trial
What if Va-1>0?A strong analysis prior CIs will be shifted towards ma If ma=0, then probability of a positive event increased 95% CIs will be narrower than for the frequentist approach
Conclusions • Bayesian approach more natural for equivalence (Can prove H0) • More work on getting pragmatic suggestions for Va and Vd needed