Download

1 / 62
670 likes | 1.07k Views
AORTIC STENOSIS AND MITRAL VALVE PROLAPSE. PRESENTED BY: FADAIRO OLUMAYOWA BEATRICE 692. AORTIC STENOSIS.

E N D
AORTIC STENOSIS ANDMITRAL VALVE PROLAPSE PRESENTED BY: FADAIRO OLUMAYOWA BEATRICE 692
Aortic valve is the valve located between the left ventricle of the heart and the aorta, the largest artery in the body which carries the entire output to the systemic circulation.
Aortic valve have 3 cusp – one located on the anterior wall(right coronary cusp)& two located in the posterior wall(left and posterior cusp)
The normal aortic valve area is approximately 3.5–4.0 cm2. Critical aortic stenosis is usually present when the area is less than 0.8 cm2.
Incidence ¼ of all with patient chronic VHD Male> female (80% of adult pt with symptomatic valvular AS are male ) It is the most common form of VHD in US
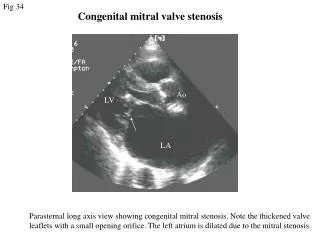
Etiology Congenital- Stenotic since birth (< 30 yr) Bicuspid – 1-2 % of population (40-60 yr ) - Male > female (3 : 1 ) - 6% have coartation of aorta - Mechanical shear stress produce injury & stenosis
Cont. Secondary to inflammation (40-60 yr ):- -Mainly rheumatic -MC cause of AS in India and world -Isolate rheumatic AS- rare (Rheumatic AS always associated with mitral valve involvement and AR ) -Post inflammation -> commissural fusion
Cont. Degenerative:- -MC cause of AS in US and EUROPE ->30% people of >65yr –have AV sclerosis -Stenosis is due to sclerosis and calcification -Progress from the base of the cusp to the leaf-lets
Rheumatic and Calcified Valves Calcific Bicuspid Valve Rheumatic Valve Calcific Tricuspid Valve
Mixed Valves Congenital Bicuspid Valve affected by Rheumatic Disease and Calcification Tricuspid Valve with Rheumatic Disease creating a functional bicuspid valve, and calcification
Aortic StenosisClues to diagnosis Aortic Stenosis Aortic Regurgitation Isolated AS or MV involvement with calcification Rheumatic under 70 yrs. Old over 70 yrs. Old bicuspid valve senile degeneration
Risk factors of AS Bicuspid aortic valve Risk factors for atherosclerosis - age - male sex - smoking - DM, HTN - ↑ LDL , ↓ HDL , ↑ CRP Rheumatic fever Conditions with ↑SV and altered calcium metabolism
Pathophysiology Aortic stenosis ↓ Obstruction to LV ejection ↓ Pressure overload ↓ ↑LV mass (↑wall thickness) ↓ ← ← ← → → → ↓ ↓ Compensated Decompensated ↓LV compliance Fibrosis:↓ contractility Normal contractility ↓ ↓ LV filling ; ↓early LV dilatation ↑late ↓ ↓ SV: normal SV: decreased
Cont. The LVH is due to increase wall tension,in accordance with Laplace”s law: Wall tension = P*R/2H p - intraventricular pressure r – inner radius h – wall thickness
Cont. Pressure overload ↓ ↑Peak systolic pressure ↓ ↑Wall tension ↓ Parallel replication of sacromeres (-) ↓ Increase wall thickness ↓ Concentric hypertrophy Concentric hypertrophy normalizes wall stress and thus preserve myocardial contractility
Cont. Consequence of LVH – - Alternation in diastolic compliance - Imbalance in myocardial supply/demand relationship - Possible deterioration of intrinsic contractile performance of myocardium
Cont. • Pressure –volume loop in AS
Cont. Increased chamber stiffness impedes early left ventricular filling Hence atrial systole is critical in maintaining ventricular filling and SV In AS atrial systole accounts for 40% of LVEDV. (Normally it contribute 15-20% of LVEDV )
Cont. • Although contractility is preserved, hypertrophied ventricle is sensitive to ischemia and LVF
Natural history Prolonged latent period Once moderate stenosis present rate of progression is – -0.3m/s jet velocity/yr -Mean pressure gradient= 7 mm-hg/yr -↓in valve area= 0.1cm2 /yr
Aortic StenosisClinical Manifestations • History • Angina • Occurs in 2/3 of patients with critical AS • Half of the patients have normal coronaries • Results from increased oxygen demand by a hypertrophied myocardium and decreased oxygen delivery secondary to compression of the vessels • Average survival is 5 years
Aortic StenosisClinical Manifestations • History • Syncope • Due to reduced cerebral perfusion • May be orthostatic, exertional, medication related (nitrates, diuretics, etc.), or due to arrhythmias • Average survival is 3 years
Aortic StenosisClinical Manifestations • History • Heart Failure • Manifest as orthopnea, dyspnea, PND, pulmonary edema • Average survival is 1 – 2 years • Microangiopathic hemolytic anemia • Sudden death
Aortic StenosisClinical Manifestations • Physical Examination • Carotid Arterial Pulse • The classic arterial pulse is called pulsusparvus et tardus(slow and late) • Precordium • The apical impulse has a sustained lift • There is little or no displacement of the Point of maximal impulse
Aortic StenosisClinical Manifestations • Physical Examination • Auscultation • S1 – usually normal, may be soft if CHF present • S2 – the intensity of A2 decreases as the valve stiffens • S2 splitting – with prolongation of LV ejection time A2 will occur later than P2 and cause paradoxical splitting of S2
Aortic StenosisClinical Manifestations • Physical Examination • S3 – usually not a normal finding in aortic stenosis, it’s presence suggests LV dysfunction • S4 – is usually present and suggests LV hypertrophy and decreased LV compliance • Ejection click occurs when the leaflets abruptly halt after maximal upward excursion and imply a mobile valve. It disappears as the valve becomes severely calcified.
Murmur of Aortic Stenosis Heard best at the 2nd RICS radiating to the carotids, sometimes throughout the precordium. S 2 S4 S 1
Aortic Stenosis Severity Mild Moderate Severe
Physical findings Delayed sustain peak of arterial pulse (pulsusparvus et tardus ) Bifid apical LV impulse Systolic thrill Late peaking Systolic ejection murmur (2nd right intercostsl space ) Paradoxical S2 S4 (with LVH ) & S3 (with LVF ) (Thrill and intensity of murmur does not correlate with severity )
Investigation CXR and ECG - LVH - Dilatation of ascending aorta - Aortic calcification
Echocardiography 2D/Doppler TTE- test of choice Provide information about- - Etiology, location - Valve gradient and area - Systolic/diastolic LV function - Coartation associated with bicuspid valve
Cardiac Catheterization Provide information about - Pressure gradient - Aortic valve area - Cardiac output
Cont. • Gradient across valve normal until orifice area reaches less than half of normal • Onset of symptoms • 0.9 cm2 with CAD • 0.7 cm2 without CAD
Aortic StenosisMedical Management All patients should follow SBE prophylaxis guidelines Avoid vigorous exercise Use nitrates and diuretics with caution Asymptomatic patients should report the onset of any symptoms promptly
Bio prosthetic valves- patient do not need an anticoagulant but it does not last long Mechanical prosthetic valve- patient will need to be using anticoagulant (warfarin) with INR of 2.0-3.0
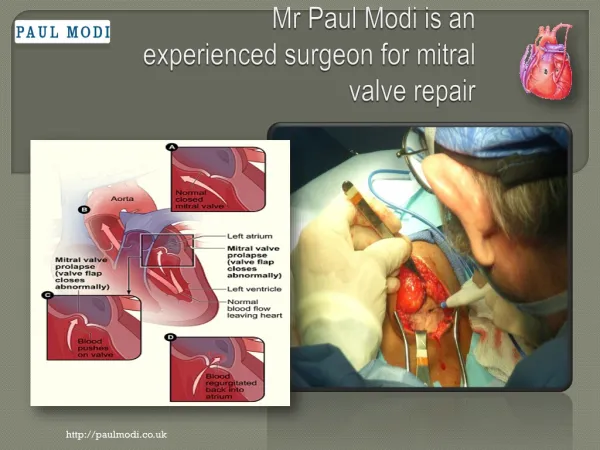
Mitral Valve • Consists of 6 major anatomical components • Annulus • Leaflets • Chordae tendinae • Papillary muscles • Posterior left atrial wall • Left ventricular free wall
Mitral Valve Prolapse: Introduction • A variable clinical syndrome that results from a diverse pathogenic mechanisms of one or more portions of mitral valve apparatus, valve leaflets, chordae tendinae, papillary muscle & valve annulus. • Many names: • Systolic click murmur syndrome • Barlow syndrome • Billowing mitral cusp syndrome • Myxomatous mitral valve syndrome • Floppy valve syndrome • Redundant cusp syndrome
Epidemiology Prevalence of 2.4% of population Twice frequent in females than in males Severe MVP occurs more frequently in older males (>50yrs)
Etiology • Primary condition • Familial – Autosomal trait • Secondary conditions • Heritable disorders of connective tissue