Download
1 / 22
280 likes | 616 Views
Management of Patients With Chronic Pulmonary Disease. COPD:. Chronic Obstructive Pulmonary Disease A disease state characterized by airflow limitation that is not full reversible (GOLD). COPD is the currently is 4 th leading cause of death and the 12 th leading cause of disability.

E N D
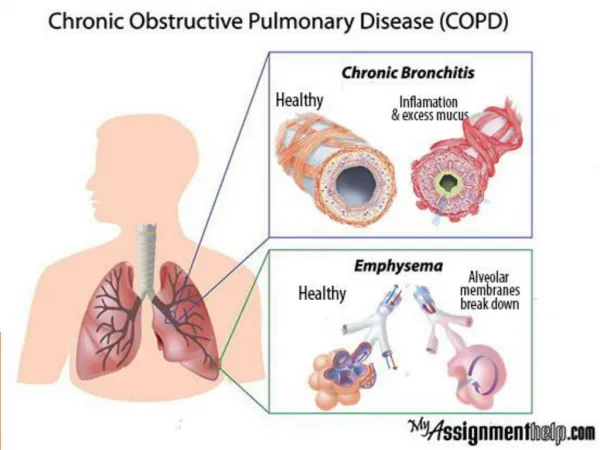
COPD: • Chronic Obstructive Pulmonary Disease • A disease state characterized by airflow limitation that is not full reversible (GOLD). • COPD is the currently is 4th leading cause of death and the 12th leading cause of disability. • COPD includes diseases that cause airflow obstruction (emphysema, chronic bronchitis) or a combination of these disorders. • Asthma is now considered a separate disorder but can coexist with COPD.
Pathophysiology of COPD • Airflow limitation is progressive and is associated with abnormal inflammatory response of the lungs to noxious agents. • Inflammatory response occurs throughout the airways, lung parenchyma, and pulmonary vasculature. • Scar tissue and narrowing occurs in airways. • Substances activated by chronic inflammation damage the parenchyma. • Inflammatory response causes changes in pulmonary vasculature.
Chronic Bronchitis • The presence of a cough and sputum production for at least 3 months in each of 2 consecutive years. • Irritation of airways results in inflammation and hypersecretion of mucous. • Mucous-secreting glands and goblet cells increase in number. • Ciliary function is reduced, bronchial walls thicken, bronchial airways narrow, and mucous may plug airways. • Alveoli become damaged, fibrosed, and alveolar macrophage function diminishes. • The patient is more susceptible to respiratory infections.
Emphysema: • Abnormal distention of air spaces beyond the terminal bronchioles with destruction of the walls of the alveoli. • Decreased alveolar surface area causes an increase in “dead space” and impaired oxygen diffusion. • Reduction of the pulmonary capillary bed increases pulmonary vascular resistance and pulmonary artery pressures. • Hypoxemia result of these pathologic changes. • Increased pulmonary artery pressure may cause right-sided heart failure (corpulmonale).
Risk Factors for COPD • Tobacco smoke causes 80-90% of COPD cases! • Passive smoking • Occupational exposure • Air pollution • Genetic abnormalities(2% of cases) • Alpha1-antitrypsin deficiency ( enzyme inhibitor that protect the lung parenchyma from injury)
Clinical Manifestation • 3 primary symptoms: • Chronic cough • Sputum production • Dyspnea on exertion • Wt loss • Barrel chest (A-P diameter/ Transverse diameter : 2/1) • Retraction in the supraclavicular area on inspiration • Shrug shoulder • Abdominal muscle contraction on inspiration (paradox respiration) .
Medical Management • Risk reduction • Pharmacologic therapy • Management of exacerbation • O2 therapy • Surgical management • Pulmonary rehabilitation
Nursing Process: The Care of Patients with COPD- Assessment • Health history • Inspection and examination findings • Review of diagnostic tests
Nursing Process: The Care of Patients with COPD- Diagnoses • Impaired gas exchange • Impaired airway clearance • Ineffective breathing pattern • Activity intolerance • Deficient knowledge • Ineffective coping
Collaborative Problems • Respiratory insufficiency or failure • Atelectasis • Pulmonary infection • Pneumonia • Pneumothorax • Pulmonary hypertension
Nursing Process: The Care of Patients with COPD- Planning • Smoking cessation • Improved activity tolerance • Maximal self-management • Improved coping ability • Adherence to therapeutic regimen and home care • Absence of complications
Improving Gas Exchange • Proper administration of bronchodilators and corticosteroids • Reduction of pulmonary irritants • Directed coughing, “huff” coughing • Chest physiotherapy • Breathing exercises to reduce air trapping • diaphragmatic breathing • pursed lip breathing • Use of supplemental oxygen
Improving Activity Tolerance • Focus on rehabilitation activities to improve ADLs and promote independence. • Pacing of activities • Exercise training • Walking aides • Utilization of a collaborative approach
Other Interventions • Set realistic goals • Avoid extreme temperatures • Enhancement of coping strategies • Monitor for and management of potential complications
Patient Teaching • Disease process • Medications • Procedures • When and how to seek help • Prevention of infections • Avoidance of irritants; indoor and outdoor pollution, and occupational exposure • Lifestyle changes, including cessation of smoking