Download
1 / 37
400 likes | 505 Views
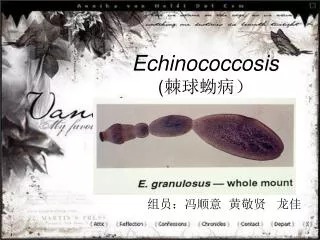
Echinococcosis (Hydatid Disease). Echinococcus granulosus Echinococcus multilocularis . Humans acquire the infection when they become intermediate hosts of these tapeworms by accidental ingestion of the eggs of Echinococcus Spp.

E N D
Echinococcusgranulosus • Echinococcusmultilocularis. • Humans acquire the infection when they become intermediate hosts of these tapeworms by accidental ingestion of the eggs of Echinococcus Spp.
After entering the body, the eggs transform into cysts that grow in tile liver, lungs, heart, and CNS . • In the latter, cysts may also result from metastatic dissemination of a visceral cyst.
Cystic Hydatid Disease (Echinococcus granulosus) • Seizures. • increased intracranial pressure. • focal neurological deficits. • Orbital involvement : proptosis and ophthalmoplegia
Diagnosis • large non enhancing vesicle that is well demarcated from the surrounding brain parenchyma. • Some lesions may be calcified. • epidural cysts have a biconvex shape or a multilocular appearance and may be associated with bone erosion.
Giant" cysticercal cyst in the right sylvian fissure“ Intraventricular cysticercus
Diagnosis • enzyme-linked immunosorbent assay (ELISA) • enzyme-linked immunoelectrotransfer blot (EITB) • false-negative results in up to 50%.
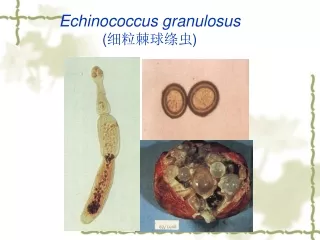
Pathology • E. granulsus cysts are large, spherical, and well demarcatedfrom surrounding tissue. • within the CNS, these cysts may be located in the brain parenchyma, ventricular system, subarachnoid space, epidural space, orbits, and both the epidural and subarachnoid spaces in the spinal canal.
Pathology • epidural cysts tend to be associated with vertebral bone erosion. • Primary hydatid disease of the heart may be the source of an embolic cerebral infarction, usually in the territory of the middle cerebral artely.
Treatment • Antiparasitic drugs are usually given before surgical resection in the case of intraoperative rupture of cysts or postoperatively to treat recurrent hydatid disease.
CYSTIC HYDATID DISEASE OF THE BRAIN • Dowling's technique: hydrostatic expulsion of the entire cyst by irrigation of saline solution between the lesion and the surrounding nervous tissue. • The aim of this technique is to remove the cyst without damaging its walls.
accidental intraoperative rupture • 25% of cases. • allergic reaction. • recurrent hydatid disease.
Complications: subdural effusions and intracranial hemorrhages. • some surgeons puncture the cyst,aspirate its contents, irrigate the cyst with a hypertonic salinesolution, and then remove the shrunken cyst.
Albendazole • 10 to 15 mg/kg per day. • several 1-month cycles with therapy-free intervals of 14 days between cycles. • Cured 28% of patients and improved the condition of 51% of other 72%
Albendazole • Patiens not candidates for surgical resection of lesions. • prophylactic therapy for those at risk for accidental rupture of the cysts perioperatively, • recurrent cystic hydatid disease after surgery. • combined albendazole and praziquantel tllerapy may be more effective than albendazole alone for preoperative prophylactic treatment.
CYSTIC HYDATID DISEASE OF THE SPINE • The surgical approach to patients with spinal hydatid disease usually includes a combination of : • decompressive laminectomy, • removal of cysts. • excision of involved bone. • stabilization of the spine.
Almost 50% of these lesions may rupture during surgery because of the narrow space in which the surgeon has to work. • involvement of adjacent bone and multiplicity of lesions make complete removal of spinal cysts difficult. • Hydatid disease recurs after surgery in up to 40% of patients, and this complication is associated with neurological deterioration. • albendazole is advised to reduce such complications.
Alveolar Hydatid Disease(Echinococcus multilocularis) • more rapidly • more severe • focal neurological deficits, seizures, and intracranial hypertension.
Diagnosis • On neuroimaging studies, alveolar hydatid disease is characterizednby multiple lesions surrounded by edema, with ring-like enhancement mimicking other infectious or neoplastic diseases of the CNS. • CT is better than MRI for demonstrating lytic lesions in vertebral bodies. • Immunologic diagnosis is better with alveolar echinococcosis than with cystic hydatid disease.
Pathology • E. Multilocularis cysts are small, group in clusters, elici t a severe • Infiammatory reaction from the host, and tend to metastasize both locally and distantly • They are usually located within the brain parenchyma. • Primary hydatid disease of the heart may be the source of an embolic cerebral infarction that is generally located in the territory of MCA
Treatment • Alveolar hydatid disease is invasive, and total surgical removal usually requires resection of adjacent tissue. This approach may cause neurological deficits from cysts located in eloquent cerebral areas. • Albendazole may be used as primary therapy in patients with inoperable alveolar hydatid disease.
With a combination of surgery and "cysticidal therapy, 50% of lesions regress, 40% remain static, and 10% continue to grow.