Download
1 / 9
90 likes | 189 Views
Follow the Placement Monitoring Team's journey in implementing interventions for a complex case study involving a female service user with LD, mental health issues, and autism. Learn about the challenges, progress, and future considerations.

E N D
Placement Monitoring Team: Interventions & Observations of a Lambeth Case Study Heidi Emery MHLD Placement Coordinator Placement Monitoring Team (PMT) MHLD Services South London and Maudsley NHS Foundation Trust NHS Foundation Trust
Service Users – Learning Disabilities, Mental Health/Complex/Forensic needs. Majority subject to Mental Health Act (2007)or complex MCA issues .In Medium, Low Secure Units / Specialist Community placements > £100,000 per year but < £ 200,000 in most cases Long term input required due to complex needs and requirement for creative and complex rehabilitation programmes Background for Out of Area Service Users
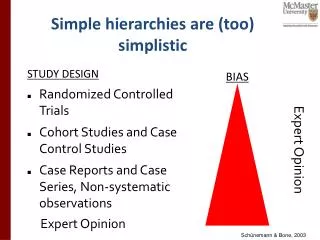
Case Study: • Female. • 45 years old. • Diagnosis: Mild LD, Bi-Polar Affective Disorder, Autism and Epilepsy. • 11 Years placed out of area. • 11 Years held under MHA 1983 Section 3. • No forensic History, though high level of care staff assaults.
Initial Assessment – a picture of some issues: • No display of picture easy-read service user information on the ward • Copies others' behaviour and wants attention approximately 4 times an hour • Unsettled since Christmas when her mother went away on holiday and was subsequently unable to come and see her due to bad weather in the winter. • Misses out on activities due to aggressive and unpredictable behaviour • No relationships with her peers and only the qualified staff. • No interaction with community-based projects only going out for walks and meals with two escorts.
Example Concerns from Initial Assessment: • Care plans had remained the same since early in the admission except for seizures plan which was discontinued. • No up-to-date assessments of her psychological presentation and assessment of her IQ. • Little change in ward round monthly records. • No clear planned evidence of discharge planning. • Living skills and lifestyle management/rehabilitation not a focus of the admission. • Minimal Occupational Therapy input and when activities stopped they were not readily replaced.
12 months later, PMT take on the case: • Placement was very inflexible with organising dates for meetings so all parties could attend. • Little change from previous assessment 12 months ago. • Lack of recognition that suitable treatment options were not available. • MHRT directions not adhered to with subsequent ruling to move to an alternative placement.
Placement Reported to CQC on the following concerns: • Family not invited to S117 discharge planning meeting. • Placement ignored recommendations of transition plan. • Belief that having 3 patients on the ward with learning disability equated to providing an LD service. • No appropriately trained staff to provide such LD service. • Poor and defensive communication with external parties when rationales questioned.
Future for the Service User: • She has moved to a hospital where her LD and Autism needs can be met with appropriate treatment options available.( Placement is now in London) • Family are engaged. • Care pathway being considered as an ongoing issue, and opportunities for rehabilitation into the community being planned for • Some incidents but less in severity and patient appears much happier. • High level of Psychology input.
Further Information: • Please feel free to contact me to discuss any issues in this presentation: • Heidi.Emery@slam.nhs.uk • Tel: 07800662407